Lecture
As a special science, neurolinguistics took shape by the middle of our century. In our country, the father of this branch of knowledge is A. R. Luria. However, the formation of this new branch of knowledge was preceded by more than a century of accumulation of data on speech disorders in local brain lesions - aphasia. The emergence of neurolinguistics was also prepared by the successful development of neurology, psychology and linguistics. We can say that neuro-and psycholinguistics have common origins. Having arisen at the same time, both these sciences are closely intertwined with a commonality of problems and the subject of study, complementing each other with data obtained in different ways.
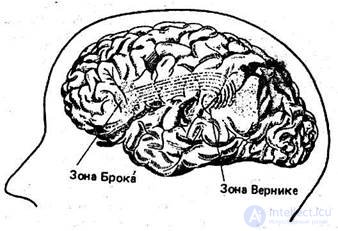
The history of studying violations of various forms of speech activity in local brain lesions begins its countdown in 1861, when French anatomist Broca showed that a lesion in the posterior third of the first frontal gyrus of the left hemisphere leads to a kind of pathology in which the patient loses the ability to speak, although completely retains the ability to understand the speech addressed to him. The region of the cerebral cortex
ha, open to scientists began to be called the center of Broca; Aphasia associated with a violation in this area, became known as motor aphasia.
Thirteen years later, in 1874, the German psychiatrist K. Wernicke described a second fact of no less significance. He showed that patients with a lesion in one third of the first temporal gyrus of the left hemisphere retain the ability to speak, but lose the ability to understand the speech facing them. Aphasia, caused by a violation in the Wernicke zone, was called sensory aphasia. These discoveries laid the foundation for a clinical study of the cerebral organization of human speech activity. Already in the early stages of the development of aphasiology, preliminary conclusions were made.
1. The speech process is based on a number of jointly working zones of the cerebral cortex, each of which has its own specific meaning for the organization of speech activity. From here the conclusion about the need for further searches for new zones responsible for other communicative functions was involuntarily suggested.
2. Both speech zones are adjacent to more general areas of activity: the center of Broca is adjacent to the motor area, and the center of Wernicke is adjacent to the auditory one. This observation gave rise to the assumption that speech control zones correlate with much more general brain behavior control zones.
3; The Broca and Wernicke zones are located in the left hemisphere of the brain. Violations in the right hemisphere, as a rule, do not entail speech anomalies. This led to the declaration of the left hemisphere "dominant", the most human, and the right one - something like atavism, the heritage of the animal state of man.
After the discoveries of Brock and Wernicke, scientists enthusiastically set about finding new speech zones. Some researchers thought that sooner or later an accurate map of the brain could be made, which would indicate narrowly limited areas that provide such aspects of speech as sound recognition, lexical, morphological or syntactic level of speech activity. A similar position was taken, for example, by the famous German psychiatrist Kleist. Failures in the implementation of such experiments led to other extremes: there were suggestions that localization provided almost nothing for understanding the mechanisms of speech. It turned out that the data
linguistics is poorly linked to the speech functions of the brain areas opened by physiologists. Gradually, the initially emerging optimism was replaced by skepticism.
However, the data accumulated, the study of the "language-brain" system continued. A significant number of observations of various types of aphasia were made during World War II. Here we must once again note the great importance of the work of A. R. Luria, who during the war was the chief specialist of the Red Army in restoring the activities of soldiers and officers who suffered a brain injury. It was during these years that he collected and summarized a great deal of material, the analysis of which was used as the basis for the new science of neurolinguistics. Luria and his students (T.V. Akhutina, E.D. Chomskaya, L.S. Tsvetkova, and many others) studied in detail the linguistic functions of the left hemisphere. Therefore, we will begin consideration of the cerebral organization of human speech activity from this particular area of the brain.
The zones opened by Broca and Wernicke, as can be seen in the figure, are located in the central and middle parts of the brain. The human brain is different from the brain of Pithecanthropus and Neanderthal by the enlarged frontal and occipital regions. It is logical to assume that it is here that the most "human" centers are located, including the centers responsible for speech.
Lesions of the deep parts of the brain can cause the destruction of the motivational basis of speech. In this case, the patient is in a state of inhibition and does not feel the desire to enter into communicative contact with anyone. Violations in the area of the primary design of the motive, the disintegration of speech programming and control of the process of speech activity are observed with severe bilateral lesions of the frontal lobes of the brain. Patients in this case retain the ability to construct a statement, but their speech either assumes the character of an echolalic repetition of a given question, or slips into a chain of side associations. For example, when fulfilling the task of reproducing the story “Chicken and Golden Eggs”, the patient easily repeats the first phrase “One owner had a hen that laid golden eggs”, then gets distracted by extraneous reasoning, then reaching the place where it is said that that the owner killed the chicken and did not find gold inside it, he begins to say: “He opened the chicken, then closed the chicken, then opened, then closed ... the door opens, the door closes ... so I enter the dining room, sit at the table ... ".
Before we talk about other speech disorders, we recall that the structure of any national language (as well as language activity) relies on two basic mechanisms; the mechanism of syntagmatics (combining elements of the linguistic structure into a linearly organized utterance, coherent speech) and the mechanism of paradigmatics (responsible for selecting the necessary component - phonetic, lexical, morphological - from a variety of similar forms). How does the structure of the language and the device of the left hemisphere of the brain?
Clinical observations have shown that violations of the anterior divisions of the speech zones lead to the disintegration of the syntagmatic mechanisms of speech production. In this case, the patient retains the ability to pronounce words, but cannot form a coherent message. Speech disorders caused by lesions of the frontal portions of the brain are sometimes characterized by a “telegraphic-style” syndrome, when aphasic either utters individual nouns, or is limited to jerk-off sentences. An example of such a speech is a story about the history of his injury: “ Here ... here .., front ... here ... offensive ... here ... here ... bullet ... here ... nothing .. here ... hospital ... operation ... here ... speech ... speech ... speech ... ".
Another example is the story “F. Two Again” by F. P. Reshetnikov:
- Boy ... mother ... The boy brought a two ... Well ... brother ... well, a bicycle ... and my sister writes ... well ... well, that's it.
- Describe the room.
-Good ... Well ... The table and everything ... a chair and a buffet, well, that's all.
- Why did the boy get a deuce?
-Skates.
Other cases of violation of the frontal regions of the left hemisphere cause a violation of coherent speech in general, when instead of a coherent text, the patient is limited to individual cliche sentences. So, one of the aphasics with a similar violation during the assignment to compile an oral essay on the topic “North” after a long pause said: “ Bears live in the north ”. Then he thought and added: “ What I bring to your attention .” Another patient simply read a phrase from a poem by M. Yu. Lermontov: “In the north, wild stands alone on the bare top of a pine tree.”
As the observations of scientists show, with the defeat of the frontal or anterior parts of the speech zone, violations are manifested mainly in the process of generating the utterance. Here, the processes of deployment of the semantic program in internal speech usually suffer: either the formation of a common idea into a sequential speech message scheme, or the construction of a coherent text.
Completely different disorders of speech activity occur in the defeat of the posterior parts of the left cerebral cortex, including the temporal and parieto-occipital parts of the brain. In this case, the paradigmatic mechanisms of generating and understanding the utterance suffer. At the level of the formation of the message, this finds expression in the fact that the patient has difficulty in choosing linguistic units at various levels: phonemes, word forms, words. For example, some of this kind of aphasics are confused in the selection of sounds: instead of a room, they pronounce the gonmada , instead of Boris - Paris . The problem of choice manifests itself at the level of the selection of the right word. In this case, the patient has difficulties in the framework of the semantic field (recall that we talked about the structure of the semantic field in the first chapter). When he is shown pictures and asked to name items drawn on them, instead of the word chest , he can say a suitcase , instead of a monkey , a parrot (the chest and the suitcase belong
they are pressed to one semantic unity - everyday objects intended for storage of things; monkey and parrot - exotic animals). The safety of the syntagmatic organization of speech in violation of its paradigmatic structure is well illustrated by the story in the picture “Accident” made by a patient with a lesion in the temporal zone:
- This is a tram, a car for the sick ... no, how ..- the janitor carries a girl, or a boy ... They are interested in women ... they are all in line, and the car leaves and they leave, they have nothing to do ... apparently, by car touched ... touched him, raised him to the hospital ... From the point of view of syntax, the speech is organized quite well, but the patient constantly forgets the words, gets confused in the selection of word forms, etc.
Damage to the posterior brain regions leads to impaired speech understanding at the stage of decoding linguistic signs: does the disintegration of the phonemic perception structure prevent it? listener to isolate the words in the speech flow, violation of the lexical-semantic composition leads to difficulties in understanding the meanings of words, etc.
Modern neurolinguistics has accumulated a rather large baggage of classifications of speech disorders arising from brain damage. One of the most common in domestic science belongs to A. R. Luria. The scientist distinguishes six forms of aphasia: (1) acoustic-gnostic (sensory ) and (2) acoustic-mnestic (they occur when the temporal regions of the cerebral cortex are damaged); (3) semantic and (4) afferent motor (occur when the lower parietal cortex of the brain is affected); (5) efferent motor and (6) dynamic (occur with the defeat of the premotor and posterior pterygomas of the cerebral cortex).
1. Acoustic-gnostic , or sensory aphasia (called Wernicke's aphasia) occurs when the posterior third of the superior temporal gyrus of the left hemisphere is affected. It is distinguished by the disintegration of ideas about the sounds of speech (phonemic hearing), as a result of which the understanding of speech suffers: patients can take one sound after another, do not understand the sound of the word (the word “kidney” perceives aphasic as “barrel”, “daughter” - as “dot " etc.).
2 Acoustic-mnestic or amnestic aphasia occurs when the middle and posterior parts of the temporal region are affected.
land In this form of speech disorder, the phonemic ear remains intact, the patient correctly perceives the sounds of the native language, understands the spoken speech to him. However, he is not able to memorize even a relatively small speech material due to the gross violation of aural-speech memory. In active speech, there is a forgetting of proper names, names and functions of objects, etc. For example, a patient can say: “ I need ... well, how is it ... so narrow ... well, what is painted ... (meaning pencil) .”
3. Semantic aphasia becomes a consequence of the lesion of the parietal-occipital region of the left hemisphere. This impaired speech is characterized by difficulties in understanding the logical-grammatical side of speech: a) patients do not see the difference in the expressions “circle above the cross”, “circle under the cross” or “cross under the circle”; b) they cannot navigate in comparative phrases such as: “Kolya is higher than Vasya. Which one is the tallest? Who is the lowest? "; c) they do not understand phrases that convey “communication of relations” like “brother of father”, “father of brother”, etc .; d) they find it difficult to understand complex syntactic constructions that convey causal, temporal and spatial relationships, implicated and participial revolutions (for example: “Before going to the city, he went to a comrade”, etc.), etc.
4. Afferent motor aphasia occurs when the lower parts of the parietal cortex are affected. In patients suffering from this type of speech pathology, the primary defect is the difficulty of distinguishing the sounds of speech that are close in articulation. As a result, aphasic either has no situational speech at all, or there are violations of the pronunciation of words, replacing one sound with another (for example, the word “robe” is pronounced like “hadat”, “elephant” - like “snol” or “elephant”, etc. ).
5. Efferent motor aphasia appears when the lower cortex of the premotor region (“Broca's zone”) is affected. In this case, patients often cannot utter almost any articulate sound. At the same time, they to some extent understand the speech addressed to them (single words and whole phrases). The milder forms of this speech violation can be characterized by agrammatism in speech production (omission of verbs, difficulties in using sentences
gov, inflection of nouns; to the grammatism of the “telegram style” type, etc.).
6. Dynamic aphasia occurs when the posterior fossa of the left hemisphere of the brain, located near the Broca area, suffers. The main speech defect in this form of speech disorder is the difficulty, and sometimes the complete impossibility of the active deployment of the utterance. Patients suffer from the ability to give a detailed speech statement, which indicates violations in the field of internal speech. This is manifested in the primitiveness of the syntactic structure, the presence of speech patterns, cliché. When drafting a story based on a picture, while retelling the text, separate, unrelated fragments are pronounced, for example: " Here ... the owner had a chicken ... and golden eggs ... and he killed her ... here it is!" And t .d
In addition to the typology of Luria, there are other classifications of speech disorders in aphasia. Let us give one of the typologies of left hemispheric disorders created by foreign neurophysiologists (in terms of 1981).
1. Anemic aphasia. It is observed in case of damage to the so-called "angular gyrus" connecting the temporal, parietal and occipital lobes of the left hemisphere. It is expressed in the fact that with the intact normal understanding of someone else's and one's own speech, the patient often forgets individual words, including the most simple ones, for example, the names of loved ones. It is considered a relatively mild form of aphasia and can be cured pretty quickly.
2 “Verbal deafness” is caused by trauma to the area connecting the Wernicke zone to the auditory entrance (that is, the area of the cortex directly connected to the middle ear). With this type of aphasia, the understanding of writing, oral speech and writing itself remain normal. But the understanding of the oral speech addressed to the patient is either very difficult or completely disturbed.
3. Conductive aphasia . The fibrous structures of the cortex at the junctions of the Wernicke and Broca zones are injured. Characteristic of speech: a) someone else's speech is partially understood and own reading is partially preserved; b) the ability to correctly repeat aloud speech patterns disappears; c) in fluent own speech, many meaningless passages of words due to incorrect utterance and
broken syntactic constructs. All this is often called "verbal hash."
4. Aphasia Wernicke . It is found when the back of the first temporal gyrus is damaged, that is, the “Wernicke zone” as a whole. Consequences of violations: a) destroyed the understanding of someone else's speech; b) the patient himself retains the ability to his own, even fluent, speech, but it is filled with words that do not exist in the language; c) safe words and whole sentences grammatically (including syntax) are normative, the intonation is correct and understandable, but even in this case the content of the speech gives the impression of a strange pretentiousness. For example, the patient describes the picture of two boys stealing cookies behind the woman’s back: “Mother is not here, she does her job to get her better, but when she looks, the two boys look elsewhere. And she works another time "; d) reading and writing violated. The famous composer Maurice Ravel, suffering from this kind of aphasia after an injury in a car accident, was no longer able to play, sing properly, record his music and read a musical notation. But he could listen to music and understand it, tried to express his thoughts and emotions in connection with it.
5. Aphasia Broca . Occurs with an injury of the frontal lobe of the left hemisphere, i.e., the Broca zone. Speech symptoms: a) understanding of someone else's speech, reading and his own letter are not violated; b) his own oral speech is flawed, reveals the so-called "telegraphic style" (with the omission of official words and most verbs). The ability to clear articulation is severely impaired. Interestingly, in this aphasia, the patient is aware of his defect, whereas in the case of Wernicke's aphasia, the aphathic defect of speech is not recognized.
6. Тотальная (глобальная) афазия. Вызывается обширной травмой левого полушария коры, охватывая зоны Вернике и Брока. Наблюдается при этом полная дисфункция речевой способности (по Павлову - разрушена 2-я сигнальная система в целом). Интеллект и способность к несловесному творчеству могут быть сохранены. Именно это и имело место при тотальной афазии у покойного композитора Г. А. Шапорина, продолжавшего работу над своей оперой «Декабристы» (играя на слух).

Comments
To leave a comment
Psycholinguistics
Terms: Psycholinguistics