Lecture
Types of emotions and their general characteristics. Sensual tone of sensation. The ratio of the concepts of "emotions" and "feelings." The main characteristics of emotions. The main types of emotions. The classification of emotions. Ambivalence of emotions. Higher feelings. The main characteristics of moods.
Physiological basis and psychological theory of emotions. The problem of emotions in the XVIII-XIX century. Concepts I. F. Herbart, V. Wundt. The concept of the origin of emotions Charles Darwin. James's Theory of Emotion — Lange. The theory of emotions W. Cannon. Lindsay-Hebba activation theory. Theory of cognitive dissonance by L. Festinger. Informational concept of emotions P. V. Simonov. The physiological basis of emotions. The role of the second signal system in the formation of emotions.
The development of emotions and their importance in human life. Organic needs as primary stimulators of emotional manifestations in children, factors causing the formation of positive and negative emotions, frustration as a mechanism for the formation of emotions. The role of adults in the formation of emotions and emotional states in children. Patterns of formation of higher feelings. The role of emotions in the regulation of behavior. The main functions of emotions. Individual differences in emotional manifestations .
Everything that we encounter in everyday life causes us a certain attitude. Some objects and phenomena make us sympathetic, others, on the contrary, disgust. Some cause interest and curiosity, others - indifference. Even those individual properties of objects, information about which we receive through sensations, such as color, taste, smell, are not indifferent to us. Feeling them, we feel pleasure or displeasure, sometimes distinctly expressed, sometimes barely noticeable. This peculiar coloring of sensations, which characterizes our attitude to the individual qualities of the object, is called the sensual tone of sensations.
A more complex attitude towards oneself is caused by life facts, taken in their entirety, in the whole diversity of their properties and characteristics. Relationships to them are expressed in such complex sensory experiences, as joy, grief, sympathy, neglect, anger, pride, shame, and fear. All these experiences are feelings or emotions.
Emotions characterize human needs and the objects to which they are directed. In the process of evolution, emotional feelings and states were biologically fixed as a way to maintain the life process in its optimal boundaries. Their importance to the body is a warning about the destructive nature of any factors. Thus, emotions are one of the main mechanisms of regulation of the functional state of the body and human activity.
However, you should pay attention to the fact that we use two concepts:
"feelings and emotions". And how identical are these concepts? Is not one of them derived from the other?
The fact is that emotions are a broader concept, but feelings are one of the manifestations of emotional experiences. In practical life, by emotions we usually understand the most diverse reactions of a person - from the violent explosions of passion to subtle shades of moods. In psychology, under the emotions understand the mental processes occurring in the form of experiences and reflecting the personal significance and assessment of external and internal situations for human life. Consequently, the most essential characteristic of emotions is their subjectivity.
Due to emotions, a person is aware of his needs and the objects to which they are directed. Another universal feature of emotions that needs to be said is their assistance in fulfilling needs and achieving certain goals. Since any emotion is positive or negative, a person can judge the achievement of a goal. Thus, a positive emotion is always associated with obtaining the desired result, and a negative one, on the contrary, with failure to achieve a goal. Thus, we can conclude that emotions are directly related to the regulation of human activity.
Most emotional states affect the characteristics of human behavior, and therefore they can be studied using not only subjective, but also objective methods. For example, reddening or blanching of a person’s skin in a certain situation may indicate his emotional state. Changes in the level of adrenaline in the blood and much more can also indicate an emotional state.
Emotions are very complex mental phenomena. The following types of emotional experiences are usually attributed to the most significant emotions: affects, emotions, feelings, moods, emotional stress.
Affect is the most powerful type of emotional reaction. Affects are intense, violently flowing and short-term emotional flashes. Examples of passion can be strong anger, rage, horror, violent joy, deep grief, despair. This emotional reaction completely captures the human psyche, connecting the main stimuli with all adjacent, forming a single affective complex that predetermines a single reaction to the situation as a whole.
One of the main features of the affect is that this emotional reaction imposes on the person the need to perform an action, but at the same time the person loses a sense of reality. He ceases to control himself and may not even be aware of what he is doing. This is due to the fact that, in the heat of passion, there is an extremely strong emotional arousal, which, affecting the motor centers of the cerebral cortex, turns into motor excitation. Under the influence of this excitement, a person makes abundant and often erratic movements and actions. It also happens that in the heat of passion a person becomes numb, his movements and actions completely stop, he seems to be deprived of speech.
Similar phenomena can be observed in various natural disasters and technological disasters. For example, one of the victims of the earthquake in Armenia described this event as follows: “I never felt so helpless in my life ... People were petrified and did not move ... Then people ran without a goal. Those in the park fled in the direction of the buildings, although it was absolutely impractical. They fled to save their lives and screamed like crazy. Those who were in the houses fled to the parks. Everyone was in a panic. ”
In the state of affect, the functioning of all mental processes changes. In particular, the indicators of attention change dramatically. Its switchability decreases, and only those objects that are directly related to the experience fall into the field of perception. The attention is focused on them so much that they are unable to switch to something else. All other stimuli that are not related to the experience are not in the field of a person’s attention, they are not sufficiently aware of this, and this is one of the reasons for the uncontrollability of human behavior in the heat of passion. In the state of affect, it is difficult for a person to foresee the results of his actions, since the nature of the processes of thinking changes. The ability to predict the consequences of their actions is sharply reduced, as a result of which expedient behavior becomes impossible.
It would be wrong to think that in the state of affect a person is not at all aware of his actions, he cannot correctly evaluate everything that is happening. Even with the strongest affect, a person is more or less aware of what is happening to him, but at the same time some people can master their thoughts and actions, while others cannot. This is due to various reasons, but primarily because of the level of emotional-volitional stability, that is, because of the peculiarities of the emotional sphere and the level of development of the volitional characteristics of a person. It should be noted that this characteristic is very indicative of the behavioral regulation of people. It is connected, on the one hand, with the genetic characteristics of the organism of a particular person, and, on the other hand, with the characteristics of his upbringing.
The next group of emotional phenomena are actually emotions. Emotions are different from affects by duration. If the affects are mostly of a short-term nature (for example, a flash of anger), then emotions are more lasting states. Another distinctive feature of emotions is that they represent a reaction not only to current events, but also to probable or recalled ones.
In order to understand the essence of emotions, it is necessary to proceed from the fact that most of the objects and phenomena of the external environment, acting on the senses, cause us complex, multifaceted emotional sensations and feelings, which can include both pleasure and displeasure at the same time. For example, the memory of something unpleasant for us may simultaneously with a heavy feeling and cause joy from the consciousness that this unpleasant is left somewhere in the past. The combination of positive and negative tinges of emotional experiences is very vividly observed when overcoming the difficulties that we have to deal with. The actions themselves, which are performed in these cases, often cause unpleasant, heavy,
sometimes painful feelings, but the success we achieve is inextricably linked with positive emotional experiences.
In addition to pleasure and displeasure in many situations, there is a feeling of some kind of tension, on the one hand, permission or relief, on the other. At critical moments of activity, at crucial moments of decision making, in overcoming difficulties, in all cases when we do something important that affects us, we experience stress. Very often, this tension has a pronounced active character, accompanied by increased attention to the object of activity, a peculiar tide of mental and physical strength, a thirst for action, and special excitement that embraces us. Sometimes, when we are poorly mastered our actions, it is expressed in a kind of constraint, retarded movements, in the narrowness of perception, in an inadequate distribution of attention.
Another manifestation of emotional processes is the excitement of pushing. An excited emotional state is usually active, associated with an activity or preparation for it. Excessive arousal can, however, upset expedient activity, making it erratic, chaotic. Calm is associated with a decrease in activity, but also serves as the basis for its expedient use.
From the point of view of influence on human activity, emotions are divided into sthenic and asthenic. Stenicial emotions stimulate activity, increase the energy and tension of a person’s forces, induce him to act, say. In this case, the person is ready "mountains turned upside down." And vice versa, sometimes experiences lead to stiffness, passivity, then they talk about asthenic emotions. Therefore, depending on the situation and individual characteristics, emotions can influence behavior differently. Thus, a person experiencing a feeling of fear may have increased muscular strength, and he may rush into danger. The same feeling of fear can cause a complete breakdown, for fear he can "bend his knees."
It should be noted that attempts were repeatedly made to highlight the main, “fundamental” emotions. In particular, it is customary to single out the following emotions:
Joy is a positive emotional state associated with the ability to adequately satisfy an actual need.
Surprise - an emotional reaction that does not have a clearly expressed positive or negative sign to circumstances that have suddenly arisen.
Suffering is a negative emotional state associated with the received reliable or seemingly such information about the impossibility of satisfying the most important vital needs.
Anger is an emotional state, negative in sign, usually occurring in the form of affect and caused by the sudden appearance of a serious obstacle to the satisfaction of an extremely important need for the subject.
Disgust - a negative emotional state caused by objects (objects, people, circumstances, etc.), contact with which comes into sharp contradiction with the ideological, moral or aesthetic principles and attitudes of the subject.
Contempt is a negative emotional state that arises in interpersonal relationships and is generated by the disagreement of life attitudes, attitudes and behavior of a subject with attitudes, attitudes and behavior of the object of feeling.
Fear is a negative emotional state that appears when a subject receives information about a real or imaginary danger.
Shame is a negative state, expressed in the awareness of the inconsistency of one's own thoughts, actions and appearance, not only with the expectations of others, but also with one's own ideas about the proper behavior and appearance.
It should be noted that emotional experiences are ambiguous. The same object can cause an inconsistent, contradictory emotional relationship. This phenomenon is called ambivalence (duality) of feelings. Ambivalence is usually caused by the fact that certain features of a complex object affect the needs and values of a person in different ways.
Feelings are another kind of emotional state. The main difference between emotions and feelings is that emotions, as a rule, have the character of an orienting reaction, i.e. they carry primary information about the lack or excess of something, so they are often vague and not sufficiently conscious (for example, a vague sense of something or). Feelings, on the contrary, are in most cases objective and specific. The phenomenon of “vague feeling” (for example, “vague torment”) speaks of the ambiguity of feelings and can be viewed as a process of transition from emotional sensations to feelings. Another difference in emotions and feelings is that emotions are more associated with biological processes, and feelings with the social sphere. Another significant difference in emotions and feelings that you need to pay attention to is that emotions are more connected with the unconscious, and feelings are most represented in our consciousness. In addition, the feelings of a person always have a certain external manifestation, and emotions often do not have.
Feelings are even longer than emotions, mental standing, having a clearly expressed subject character. They reflect a steady relationship to any specific objects (real or imagined). A person cannot experience feelings at all if they are not related to anyone or anything. For example, a person is not able to experience a feeling of love if he does not have an object of affection. In the same way, he cannot feel hatred if he does not have what he hates.
Feelings arose and were formed in the process of cultural and historical development of man. Ways of expressing feelings varied depending on the historical epoch. In the individual human development, feelings act as a significant factor in the formation of the motivational sphere. A person always seeks to engage in the type of activity and the work that he likes and causes him positive feelings.
Feelings play a significant role in building contacts with other people. A person always prefers to be in a comfortable environment, rather than
in conditions that cause him negative feelings. In addition, it should be noted that feelings are always individual. What one likes may cause negative feelings to another. This is explained by the fact that feelings are mediated by the value system of a particular person.
A special form of experience is the higher feelings, which embody all the wealth of truly human relationships. Depending on the subject area to which they relate, feelings are divided into moral, aesthetic, intellectual.
Moral, or moral, are feelings that people experience when they perceive the phenomena of reality and compare these phenomena with the norms developed by society. The manifestation of these feelings suggests that the person has learned moral norms and rules of behavior in the society in which he lives. Moral norms are formed and changed in the process of the historical development of society depending on its traditions, customs, religion, dominant ideology, etc. The actions and actions of people, corresponding to the views on morality in a given society, are considered moral, moral; acts that do not correspond to these views are considered immoral, immoral. К нравственным чувствам относят чувство долга, гуманность, доброжелательность, любовь, дружбу, патриотизм, сочувствие и т. д. К аморальным можно отнести жадность, эгоизм, жестокость и т. д. Следует отметить, что в различных обществах эти чувства могут иметь некоторые различия в содержательном наполнении.
Separately, we can highlight the so-called moral and political feelings. This group of feelings manifests itself in emotional attitudes towards various public institutions and organizations, as well as towards the state as a whole. One of the most important features of moral and political feelings is their effective nature. They can act as motivating forces for heroic deeds and actions. Therefore, one of the tasks of any state system has always been and remains the formation of such moral and political feelings as patriotism, love for the Motherland, etc.
The next group of feelings are intellectual feelings. Intellectual feelings are experiences that arise in the process of human cognitive activity. The most typical situation that gives rise to intellectual feelings is a problem situation. Success or failure, ease or difficulty of mental activity cause a whole range of experiences in a person. Intellectual feelings not only accompany human cognitive activity, but also stimulate, strengthen it, influence the speed and productivity of thinking, the content and accuracy of the knowledge obtained. The existence of intellectual feelings - surprise, curiosity, inquisitiveness, a feeling of joy about a discovery made, a feeling of doubt in the correctness of a decision, a feeling of confidence in the correctness of a proof - is a clear evidence of the relationship between intellectual and emotional processes. In this case, feelings act as a kind of regulator of mental activity.
Aesthetic feelings represent a person's emotional attitude to the beautiful in nature, in people's lives and in art. Observing the objects and phenomena of reality that surround us, a person can experience a special feeling of admiration for their beauty. A person experiences especially deep emotions when perceiving works of fiction, music, fine art, drama and other types of art. This is due to the fact that they specifically intertwine both moral and intellectual feelings. An aesthetic attitude is manifested through different feelings - delight, joy, contempt, disgust, melancholy, suffering, etc.
It should be noted that the considered division of feelings is quite conditional. Usually, the feelings experienced by a person are so complex and multifaceted that it is difficult to classify them into any one category.
Many authors attribute passion to the highest manifestation of feelings - another type of complex, qualitatively unique and only human emotional states. Passion is an alloy of emotions, motives, feelings, concentrated around a certain type of activity or object. S. L. Rubinstein wrote that "passion is always expressed in concentration, concentration of thoughts and forces, their direction towards a single goal... Passion means impulse, enthusiasm, orientation of all aspirations and forces of the individual in a single direction, their concentration on a single goal" (Rubinstein S. L., 1998).
Another group of emotional states are human moods. Mood is the longest, or "chronic", emotional state that colors all behavior. Mood differs from emotions by its lower intensity and lesser objectivity. It reflects an unconscious generalized assessment of how circumstances are developing at the moment. Mood can be joyful or sad, cheerful or depressed, cheerful or depressed, calm or irritated, etc.
Mood significantly depends on the general state of health, on the work of the endocrine glands and especially on the tone of the nervous system. The reasons for this or that mood are not always clear to a person, and even more so to the people around him. It is not for nothing that they talk about unaccountable sadness, causeless joy, and in this sense, mood is an unconscious assessment by a person of how favorable the circumstances are for him. In this, moods are similar to emotions proper and are close to the sphere of the unconscious. But the reason for the mood always exists and can be realized to one degree or another. It can be the surrounding nature, events, the activity being performed and, of course, people.
Moods can vary in duration. The stability of mood depends on many factors - the age of a person, the individual characteristics of his character and temperament, willpower, the level of development of the leading motives of behavior. Mood can color a person's behavior for several days and even weeks. Moreover, mood can become a stable personality trait. It is this feature of mood that is implied when people are divided into optimists and pessimists.
Moods are of great importance for the effectiveness of the activity that a person is engaged in. For example, it is known that the same work in one mood can seem easy and pleasant, and in another - hard and depressing. Naturally, when in a good mood, a person is able to do a much greater amount of work than when in a bad mood.
Mood is closely related to the relationship between a person’s self-esteem and the level of his or her aspirations. People with high self-esteem often have an elevated mood, while people with low self-esteem have a pronounced tendency toward passive-negative emotional states associated with the expectation of unfavorable outcomes. Therefore, mood can become the reason for refusing to act and further reducing aspirations, which can lead to a refusal to satisfy this need.
The presented characteristics of the types of emotional states are quite general. Each of the
numerical types have their own subtypes, which will differ in intensity, duration, depth, awareness, origin, conditions of occurrence and disappearance, impact on the body, dynamics of development, direction, etc.
Speaking about the classification of emotional states, we did not note the fact that there have been repeated attempts to identify features common to all emotional states. One of such attempts belongs to W. Wundt. According to Wundt, the entire system of feelings can be defined as a variety of three dimensions, in which each dimension has two opposite directions that exclude each other. This coordinate system can be represented graphically (Fig. 16.1). It characterizes the sign of emotions, the degree of excitement and tension, but this approach no longer corresponds to the information accumulated in the process of studying emotions. For example, in the coordinate system proposed by W. Wundt, there is no such characteristic as the duration of the emotional reaction.
There is another special type of emotional states - emotional stress. We will consider it in the section "Mental States".
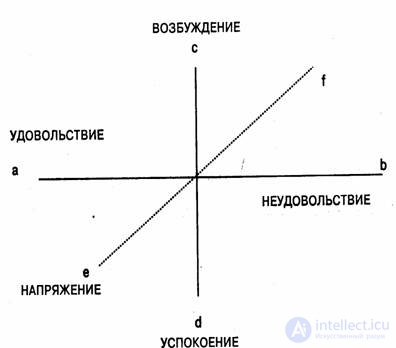
Fig. 16.1. Основные измерения эмоциональных процессов и состояний (по В. Вундту).
16.2. Physiological bases and psychological theories of emotions
It is no coincidence that this section of the chapter combines two aspects in its title:
physiological bases and psychological theories of emotions. Historically, the desire to find the root cause of emotional states has led to the emergence of various points of view, which were reflected in the corresponding theories. For a long time, psychologists have tried to resolve the issue of the nature of emotions. In the 18th-19th centuries, there was no single point of view on this problem. The most widespread was the intellectualistic position, which was based on the assertion that organic manifestations of emotions are a consequence of mental phenomena. The clearest formulation of this theory was given by I. F. Herbart, who believed that the fundamental psychological fact is a representation, and the feelings we experience correspond to the connection that is established between different representations, and can be considered as a reaction to a conflict between representations. Thus, the image of a deceased acquaintance, compared with the image of this acquaintance as still alive, gives rise to sadness. In turn, this affective state involuntarily, almost reflexively causes tears and organic changes that characterize grief.
W. Wundt also adhered to this position. In his opinion, emotions are, first of all, changes characterized by the direct influence of feelings on the flow of ideas and, to some extent, the influence of the latter on feelings, and organic processes are only a consequence of emotions.
Thus, initially, in the study of emotions, the opinion was established about the subjective, i.e. mental, nature of emotions. According to this point of view, mental processes cause certain organic changes. However, in 1872, C. Darwin published the book "The Expression of the Emotions in Man and Animals", which was a turning point in understanding the connection between biological and psychological phenomena, including in relation to emotions.
In this work, Darwin argued that the evolutionary principle is applicable not only to biological, but also to the mental and behavioral development of animals. Thus, in his opinion, there is much in common between the behavior of animals and humans. He based his position on observations of the external expression of various emotional states in animals and people. For example, he found a great similarity in the expressive bodily movements of anthropoids and children born blind. These observations formed the basis of the theory of emotions, which was called evolutionary. According to this theory, emotions appeared in the process of evolution of living beings as vital adaptive mechanisms that facilitate the adaptation of the organism to the conditions and situations of its existence. According to Darwin, bodily changes that accompany various emotional states (for example, movements) are nothing more than rudiments of real adaptive reactions of the organism, expedient at the previous stage of evolution. Thus, if hands become wet with fear, this means that at one time our ape-like ancestors had this reaction to grasp tree branches in danger. Looking a little ahead, it is necessary to say that later E. Claparède returned to this theory, who wrote:
“Emotions arise only when, for one reason or another, adaptation is difficult. If a person can run away, he does not experience the emotion of fear." However, the point of view reproduced by E. Claparede no longer corresponded to the experimental and theoretical material accumulated by that time. The modern history of emotions begins with the appearance in 1884 of the article by W. James "What is emotion?" James and, independently of him, G. Lange formulated a theory according to which the emergence of emotions is caused by changes in the voluntary motor sphere and in the sphere of involuntary acts, such as the activity of the cardiovascular system, caused by external influences. The sensations associated with these changes are emotional experiences. According to James, "we are sad because we cry; we are afraid because we tremble; we are happy because we laugh."
It is organic changes according to the theory of James-Lange that are the root causes of emotions. Reflecting in the human psyche through a system of feedbacks, they generate emotional experience of the corresponding modality. According to this point of view, the changes in the body characteristic of emotions first occur under the influence of external stimuli and only then, as a consequence of them, the emotion itself occurs. Thus, peripheral organic changes, which until the emergence of the James – Lange theory, were considered as consequences of emotions, became their root cause. It should be noted that the emergence of this theory has led to a simplified understanding of the mechanisms of arbitrary regulation. For example, it was believed that unwanted emotions, such as grief or anger, can be suppressed if you deliberately commit actions that usually result in positive emotions.
However, the concept of James — Lange raised a number of objections. An alternative point of view on the relationship between organic and emotional processes was expressed by W. Cannon. He found that the bodily changes observed in the onset of various emotional states are very similar to each other and are not so diverse as to quite satisfactorily explain the qualitative differences in higher emotional experiences of a person. At the same time, the internal organs, with changes in the states of which Jam and Lange attributed the emergence of emotional states, are rather insensitive structures. They very slowly come to a state of arousal, and emotions usually arise and develop fairly quickly. Moreover, Cannon discovered that organic changes artificially induced in humans are not always accompanied by emotional experiences. The strongest argument of Cannon against the theory of James-Lange was an experiment conducted by him, as a result of which it was found that artificially caused by stopping the flow of organic signals to the brain does not prevent the occurrence of emotions. The main provisions of the discussed theories are presented in Fig. 16.2.
Cannon believed that bodily processes with emotions are biologically expedient, since they serve as a preliminary adjustment of the whole organism to the situation when it will require an increased expenditure of energy resources. At the same time, emotional experiences and corresponding organic changes, in his opinion, arise in the same brain center - the thalamus.
Later P. Bard showed that in fact both bodily changes and emotional experiences associated with them arise almost simultaneously, and of all the brain structures, not even the thalamus itself, but the hypothalamus and the central parts of the limbic system. Later in the experiments conducted on animals, X. Delgado found that with the help of electrical influences on these structures one can control such emotional states as anger and fear.
The psychoorganic theory of emotions (this is how the concepts of James — Lange and Cannon — Bard have been called) have been further developed under the influence of electrophysiological studies of the brain. As a result of the ongoing experiments

Fig. 16.2. The main provisions in the theories of James-Lange and Cannon-Bard
mental research arose Lindsay-Hebb's activation theory. According to this theory, emotional states are determined by the influence of the reticular formation of the lower part of the brain stem, since this structure is responsible for the level of activity of the organism. And the emotional manifestations, as shown by electrophysiological studies of the brain, are nothing more than a change in the level of activity of the nervous system in response to any stimulus. Therefore, it is the reticular formation that determines the dynamic parameters of emotional states: their strength, duration, variability and a number of others. Emotions, however, arise as a result of a disturbance or restoration of balance in the corresponding structures of the central nervous system as a result of the action of an irritant.
Following the theories explaining the relationship of emotional and organic processes, theories have appeared that describe the effect of emotions on the psyche and human behavior. Emotions, as it turned out, regulate human activity, revealing a well-defined influence on it, depending on the nature and intensity of emotional experience. D. O. Hebb managed to experimentally obtain a curve expressing the relationship between the level of a person’s emotional arousal and the success of his practical activity. In his studies, it was found that the relationship between emotional arousal and the effectiveness of human activity is graphically expressed in the form of a normal distribution curve. So, to achieve the highest result in the activity, both too weak and too strong emotional arousal are undesirable. The most effective activity with an average of emotional arousal. At the same time, it was found that for each particular person a certain optimal interval of emotional excitability is characteristic, which ensures maximum efficiency in work. In turn, the optimal level of emotional arousal depends on many factors, for example, on the characteristics of the activity performed and the conditions in which it occurs, on the individual characteristics of the person who performs it, and on many other things.
A separate group of theories consists of views that reveal the nature of emotions through cognitive factors, that is, thinking and consciousness.
First of all, among them should be noted L. Festinger's theory of cognitive dissonance. Its basic concept is dissonance. Dissonance is a negative emotional state that arises in a situation where the subject has psychologically contradictory information about the object. According to this theory, a positive emotional experience arises in a person when his expectations are confirmed, that is, when the actual results of the activity correspond to the intended ones and are consistent with them. At the same time, the resulting positive emotional state can be characterized as consonance. Negative emotions arise when there is a discrepancy or discord between the expected and actual results of the activity.
Subjectively, the state of cognitive dissonance is usually experienced by a person as discomfort, and he seeks to get rid of him as soon as possible. He has two ways to do this: first, change his expectations so that they
corresponded to reality; secondly, to try to obtain new information that would be consistent with previous expectations. Thus, from the point of view of this theory, the emerging emotional states are considered as the main reason for the corresponding actions and actions.
In modern psychology, the theory of cognitive dissonance is most often used to explain a person’s actions and actions in a wide variety of situations. Moreover, in the determination of behavior and the emergence of emotional states of a person, cognitive factors are given much greater importance than organic changes. Many representatives of this direction believe that cognitive assessments of the situation directly affect the nature of emotional experience.
The views of S. Schechter are close to this point of view, which has revealed the role of human memory and motivation in emotional processes. The concept of emotions proposed by S. Schechter was called cognitive-physiological (Fig. 16.3). According to this theory, the emerged emotional state, in addition to perceived stimuli and the bodily changes they engender, is influenced by a person’s past experience and his subjective assessment of the current situation. In this case, the assessment is based on the interests and needs that are relevant to him. An indirect confirmation of the validity of the cognitive theory of emotions is the influence on the person’s experiences of verbal instructions, as well as additional information, on the basis of which a person changes his assessment of the situation.
In one of the experiments aimed at proving the provisions of the cognitive theory of emotions, people were given physiologically “medicine”

Fig. 16.3. Factors of emotion in the cognitive-physiological concept
S. Schechter
neutral solution (placebo) accompanied by various instructions. In one case, they were told that this medicine would cause them to be in a state of euphoria, in the other, they would be in a state of anger. After taking the “medicine” of the subjects after some time, when, according to the instructions, it was supposed to take effect, they asked what they felt. It turned out that the emotional experiences they experienced in most cases corresponded to the instructions given to them.
The informational concept of emotions by P. V. Simonov can also be classified as cognitive. In accordance with this theory, the emotional states are determined by the quality and intensity of the actual need of the individual and the assessment he gives to the probability of its satisfaction. A person evaluates this probability on the basis of congenital and previously acquired individual experience, involuntarily comparing information about the means, time, and resources that are supposedly necessary to satisfy the need with the information received at the moment. For example, the emotion of fear develops with a lack of information about the means necessary for protection.
The approach of V.P. Simonov was implemented in the formula
E = P (And n - And s),
Where:
E - emotion, its strength and quality;
P - size and specificity of the actual need;
And n - the information needed to meet current needs;
And with - the existing information, ie, the information that a person has at the moment.
The consequences arising from the formula are as follows: if a person has no need (P = 0), then he does not feel emotions (E = 0); emotion does not arise in the case when a person in need has a full opportunity to realize it. If the subjective assessment of the probability of satisfying a need is large, positive feelings are manifested. Negative emotions arise if the subject negatively assesses the possibility of satisfying the need. Thus, conscious or unaware of it, a person constantly compares information about what is required to satisfy a need with what he has, and, depending on the results of the comparison, experiences different emotions.
The results of experimental studies suggest that the cerebral cortex plays a leading role in the regulation of emotional states. IP Pavlov showed that it is the cortex that regulates the flow and expression of emotions, controls all phenomena in the body, has an inhibiting effect on the subcortical centers, controls them. If the cerebral cortex enters a state of excessive excitation (when overworked, intoxicated, etc.), then the centers lying below the cortex will also be overexcited, as a result of which the usual restraint disappears. In the case of the spread of widespread inhibition, depression, weakening or stiffness of muscular movements, decay of cardiovascular activity and respiration, etc. are observed.
|
It is interesting What does a person's emotion consist of? Any emotion always has several components. One of them is recognized by us as a subjective experience. The second component is the reaction of the organism. For example, when you are excited, your voice may tremble or rise against your will. The third component is the totality of thoughts that accompany the emotion and come to mind. The fourth component of emotional experience is a special facial expression. For example, if you are unhappy, you are frowning. The fifth component is associated with generalized emotional reactions. For example, with a negative emotion, your attitude towards the events around you becomes negative, the world view can “darken”. The sixth component is the propensity for actions that are associated with a given emotion, that is, the tendency to behave as people usually behave when experiencing a particular emotion. Anger, for example, can lead to aggressive behavior. By itself, none of the above components is actually an emotion. When a certain emotion arises, all these components appear simultaneously. Moreover, each of the components can influence other components. So, a cognitive assessment of the situation can cause a particular emotion. For example, if you think that the seller is trying to deceive you, you will probably feel angry. The most important problem of modern theories of emotion is the clarification of the nature of each component and the specific mechanisms of the influence of the components on each other. In parallel with this problem, other issues are also being studied. For example, what is the contribution of autonomic nervous system reactions, knowledge and facial expression to the intensity of the emotion experienced? Do you feel angry when there is no autonomous excitement! Does the power of your anger depend on having a certain kind of thoughts or a certain facial expression? What components determine the specifics of emotions? There are other questions, but only some of them can be answered today. So, today we can with some degree of confidence consider the existence of certain physiological mechanisms of emotions. Experiencing a strong emotion, we are aware of a number of changes in the body - for example, acceleration of heartbeat and breathing, dry mouth and throat, sweating, tremors, and a feeling of weakness in the stomach. Most of the physiological changes that occur with emotional arousal are the result of the activation of the sympathetic section of the autonomic nervous system when it prepares the body for emergency action. (The autonomic nervous system is the part of the peripheral nervous system responsible for regulating the activity of the glands and smooth muscles, including the heart muscle, the blood system and the muscles of the stomach.) The sympathetic division is responsible for the following changes: increased blood pressure and heart palpitations, increased breathing, pupil dilation , an increase in sweating, a decrease in saliva secretion, an increase in the level of sugar in the blood, an increase in the rate of blood coagulation, an increase in the hairs on the skin (“goose-skin”), etc. Thus, with The impathetic section adapts the body to energy costs. When the emotion subsides, the energy-saving functions of the parasympathetic division begin to prevail, returning the body to its normal state. The work of the autonomic nervous system is triggered by certain parts of the brain, including the hypothalamus and parts of the limbic system. From them, signals are transmitted to the brain stem nuclei, which control the functioning of the autonomic nervous system. The latter directly affects the muscles and internal organs, initiating some of the changes described above in the body, and also indirectly causes other changes by stimulating the release of adrenaline hormones. Increased physiological arousal resulting from the mechanisms described above is characteristic of emotional states such as anger and fear, during which the body must prepare for action, such as a fight or a run.
|
|
in one study of war veterans with various injuries of the spinal cord, all subjects were divided into five groups depending on the nature of the damage. One group included the subjects with injuries closer to the neck with a complete loss of innervation of the sympathetic system. In the other group, the lesions were at the base of the back (at the level of the sacrum) with partially preserved innervation of the sympathetic nerves. The remaining three groups were located between these two extremes. In the course of these studies, it was found that the higher the person's spinal cord injury was localized (that is, the less feedback from the autonomic nervous system was), the less was his emotion after injury. Moreover, a decrease in autonomic excitability led to a decrease in the strength of emotional experience. Comments from patients with the highest spinal cord injury localization indicate that they may react emotionally to stimulating situations, but do not actually feel emotions. For example: "It's a kind of cold anger. Sometimes I act angry when I see some injustice. I yell and swear .... but it's not as hot as it used to be. It's mental anger." Or: "I say that I'm scared, like when I had a really hard exam at school, but I don't really feel scared: none of that tension, shaking, empty feeling in the stomach that I used to have." Thus, our subjective experiences are very closely connected with physiological processes. This raises the question: can certain physiological processes cause certain emotional processes? Today, there is no clear answer to this question. Conflicting views on this issue have existed since the emergence of two theories: Cannon's and James-Lange's, which answered this question differently. The James-Lange theory stated that since the perception of autonomic arousal (and possibly other changes in the body) constitutes the experience of emotion, and since different emotions are experienced differently, each emotion must have a distinct source of autonomic activity. Consequently, emotions differ in the source of their autonomic arousal. In the 1920s, this theory was subjected to serious criticism (especially the part related to autonomic reactions). Among the opponents of this theory, the name of the physiologist Walter Cannon stands out, who put forward three main criticisms: 1. Since the internal organs are relatively insensitive structures, internal changes occur too slowly to serve as a source of emotional experiences. 2. Artificially induced changes in the body associated with emotions - for example, an injection of epinephrine - do not cause the sensation of real emotion. 3. Autonomic arousal varies slightly in different emotional states; for example, anger makes the heart beat faster, but so does the sight of a loved one. The third argument thus clearly denies the possibility of differentiating emotions by their autonomic responses. Psychologists have attempted to refute Cannon's third proposition by making increasingly precise measurements of the subcomponents of autonomic arousal. Although several experimenters reported finding physiological patterns in various emotions in the 1950s, most researchers found little evidence to support this claim until the 1980s. However, recent studies have provided compelling evidence that autonomic patterns exist for different emotions. Subjects were asked to express six emotions—surprise, disgust, sadness, anger, fear, and happiness—following instructions about which facial muscles to contract. While they maintained their expression for 10 seconds, their heart rate, skin temperature, and other measures of autonomic arousal were measured. A series of these measurements revealed differences between the emotions. Heart rate was higher with the negative emotions of anger, fear, and sadness than with the emotions of happiness, surprise, and disgust; and the first three emotions were partly distinguished by the fact that skin temperature was higher with anger than with fear or sadness. Thus, although both anger and the sight of a loved one make the heart beat faster, only anger makes it beat much faster; and although anger and fear have much in common, anger is “hot” and fear is “cold.” However, today it is impossible to give absolute preference to one or the other position. The available experimental data are too contradictory. Most likely, the answer to such an interesting and complex question will be obtained in further research. |
The fact that the cerebral cortex plays a very important role in regulating emotional states is evidenced by clinical cases in which there is a sharp discrepancy between subjective experience and their external expression. In patients with lesions of the cerebral cortex, any stimulus can cause a completely inappropriate external reaction: bursts of laughter or streams of tears. However, when laughing, these patients feel sad, and when crying, they sometimes feel joy.
The second signal system plays a significant role in human emotional experiences, since experiences arise not only from direct influences of the external environment, but can also be caused by words and thoughts. Thus, a story read produces a corresponding emotional state. At present, it is generally accepted that the second signal system is the physiological basis of higher human feelings - intellectual, moral, aesthetic.
To date, there is no single point of view on the nature of emotions. Research aimed at studying emotions is still being intensively conducted. The experimental and theoretical material accumulated to date allows us to talk about the dual nature of emotions. On the one hand, these are subjective factors, which include various mental phenomena, including cognitive processes, features of the organization of the human value system, etc. On the other hand, emotions are determined by the physiological characteristics of the individual. It can be argued that emotions arise as a result of exposure to a certain stimulus, and their appearance is nothing more than a manifestation of human adaptation mechanisms and the regulation of his behavior. We can also assume that emotions were formed in the process of evolution of the animal world and they reached the maximum level of development in humans, since they are represented objectively at the level of feelings.
16.3. Development of emotions and their importance in human life
Emotions follow a common path of development for all higher mental functions - from external socially determined forms to internal mental processes. Based on innate reactions, the child develops a perception of the emotional state of the people around him. Over time, under the influence of increasingly complex social contacts, emotional processes are formed.
The earliest emotional manifestations in children are associated with the organic needs of the child. This includes the manifestations of pleasure and displeasure when satisfying or not satisfying the need for food, sleep, etc. Along with this, such elementary feelings as fear and anger begin to appear early. At first, they are unconscious. For example, if you pick up a newborn baby and, lifting him up, then quickly lower him down, you will see that the child shrinks, although he has never fallen before. The first manifestations of anger, associated with the displeasure experienced by children when their needs are not met, are of the same unconscious nature. For example, one two-month-old child showed fear already when looking at his father's face, deliberately distorted by a grimace. This same child had angry wrinkles on his forehead when he was teased. Sympathy and compassion also appear very early in children. In scientific and educational literature on psychology, we can find numerous examples confirming this. Thus, at the age of twenty-seven months, a child cried when he was shown a picture of a crying person, and one three-year-old boy rushed at everyone who hit his dog, declaring: "How can you not understand that it hurts."
It should be noted that positive emotions in a child develop gradually through play and exploratory behavior. For example, K. Buhler's research showed that the moment of experiencing pleasure in children's games shifts as the child grows and develops. Initially, the child experiences pleasure at the moment of receiving the desired result. In this case, the emotion of pleasure plays an encouraging role. The second stage is functional. The playing child is no longer only happy with the result, but also with the process of the activity itself. Pleasure is now associated not with the end of the process, but with its content. At the third stage, in older children, anticipation of pleasure appears. In this case, emotion arises at the beginning of the play activity, and neither the result of the action nor the performance itself are central to the child's experience.
Another characteristic feature of the manifestation of feelings at an early age is their affective nature. Emotional states in children at this age arise suddenly, proceed violently, but disappear just as quickly. More significant control over emotional behavior occurs in children only in older preschool age, when they develop more complex forms of emotional life under the influence of increasingly complex relationships with people around them.
The development of negative emotions is largely due to the instability
the emotional sphere of children and is closely related to frustration. Frustration is an emotional reaction to an obstacle in achieving a conscious goal. Frustration can be resolved in different ways depending on whether the obstacle has been overcome, whether it has been bypassed, or a substitute goal has been found. The usual ways of resolving a frustrating situation determine the emotions that arise. Frequently repeated in early childhood, the state of frustration and stereotypical forms of overcoming it reinforce lethargy, indifference, lack of initiative in some, and aggressiveness, envy, and bitterness in others. Therefore, in order to avoid such effects, it is undesirable to too often achieve the fulfillment of your demands by direct pressure when raising a child. Insisting on immediate fulfillment of demands, adults do not give the child the opportunity to achieve the goal set before him on his own and create frustrating conditions that contribute to the consolidation of stubbornness and aggressiveness in some and lack of initiative in others. More appropriate
in this case is to use the age-related feature of children, which consists in the instability of attention. It is enough to distract the child from the problematic situation that has arisen, and he will be able to complete the tasks set before him.
A study of the problem of the emergence of negative emotions in children has shown that punishment of the child, especially the measure of punishment, plays a great role in the formation of such an emotional state as aggressiveness. It turned out that children who were strictly punished at home showed more aggressiveness while playing with dolls than children who were not punished too strictly. At the same time, the complete absence of punishment has an adverse effect on the development of a child's character. Children who were punished for aggressive actions towards dolls were less aggressive outside the game than those who were not punished at all.
Along with the formation of positive and negative emotions, moral feelings are gradually formed in children. The rudiments of moral consciousness first appear in a child under the influence of approval, praise, and also censure, when a child hears from adults that one thing is possible, necessary, and must be done, while another is not allowed, impossible, or bad. However, children's first ideas about what is "good" and what is "bad" are most closely connected with the personal interests of both the child himself and other people. The principle of the social usefulness of a particular action, the awareness of its moral meaning determine the child's behavior somewhat later. Thus, if you ask four- to five-year-old children: "Why shouldn't you fight with your comrades?" or "Why shouldn't you take other people's things without asking?", the children's answers most often take into account the unpleasant consequences that follow either for them personally or for other people. For example: "You can't fight, otherwise you'll hit me right in the eye" or "You can't take other people's things, otherwise they'll take you to the police." By the end of the preschool period, answers of a different order appear: "You can't fight with your comrades because it's shameful to offend them," i.e. children increasingly develop an awareness of moral principles of behavior.
By the beginning of schooling, children have a
продолжение следует...
Часть 1 16. Mental processes . Emotions
Часть 2 test questions - 16. Mental processes . Emotions
 However, the question arises, what is the relationship between increased physiological excitability and the subjective experience of emotions? The answer to this question can give studies of individuals with damaged spinal cord. When the spinal cord is dissected or damaged, sensations coming from a place below the point of damage cannot reach the brain. Since some of these sensations are caused by the sympathetic nervous system, damage to the spinal cord reduces the proportion of autonomous excitement in the emotion experienced. In particular,
However, the question arises, what is the relationship between increased physiological excitability and the subjective experience of emotions? The answer to this question can give studies of individuals with damaged spinal cord. When the spinal cord is dissected or damaged, sensations coming from a place below the point of damage cannot reach the brain. Since some of these sensations are caused by the sympathetic nervous system, damage to the spinal cord reduces the proportion of autonomous excitement in the emotion experienced. In particular, It is interesting
It is interesting
Comments