Lecture
ignificant fluctuations in the level of human vitality (calm or intense wakefulness, sleep, etc.) are one of the important problems of psychophysiology. At the same time, this problem has an interdisciplinary character. At its center is the idea of a special phenomenon, which is called functional states (FS). This concept is widely used in physiology, psychology, ergonomics (a science that comprehensively studies the working activity of people and the conditions of its flow). Therefore, knowledge of the physiological mechanisms responsible for the functional states of the human body is of very practical importance. Nevertheless, there is still no generally accepted theory of functional states, at the same time there are several approaches to the description and diagnosis of functional states of various types.
Often, a functional state (FS) is defined as the background activity of the central nervous system, under which one or another activity is performed. However, this definition cannot be considered sufficient. Firstly, it is too general in nature and does not take into account structural and functional heterogeneity of the central nervous system. Secondly, introducing as a criterion "conditions for the implementation of activities", it narrows the range of functional states of the human body, excluding from their number all conditions that are not directly related to the activity (for example, sleep or meditation). In addition, the generalization of this definition does not allow to identify the grounds on which it is possible to differentiate various functional states of the body.
A complex approach. The emergence of the possibility of multiple registration of psychophysiological indicators (EEG, heart rate, EMG, respiratory movements, etc.) led to an understanding of functional states as a complex of behavioral manifestations that accompany various aspects of human activity and behavior. From the standpoint of a systematic approach, the FS is the result of the dynamic interaction of the organism with the external environment and reflects the state of the "organized" whole. According to this logic, a functional state is an integral complex of the available characteristics of those qualities and properties of the human body that directly or indirectly determine its activity.
Thus, the functional state is the systemic response of the organism, ensuring its adequacy to the requirements of the activity. Thus, a change in PS is a change in one set of reactions to another, all of which are interrelated and provide a more or less adequate behavior of the organism in the environment. According to this logic, the diagnosis of functional states is associated with the task of recognizing a multidimensional vector, the components of which are various physiological indicators and reactions.
It is clear that the increase in the number of components of this vector, i.e. involvement in the analysis of an increasing number of indicators and reactions, as well as their various combinations, leads to even greater granularity and difficulty analyzing the functional state. However, it is positive that each FS is characterized by its own unique combination of indicators and reactions (a single-valued multidimensional vector). At the same time, no set of indicators, even if strictly ordered and unique, makes it possible to reveal the essence of a specific functional state, since it always turns out to be only an external description and enumeration lacking a meaningful characteristic that is most important for understanding the essence of FS.
Ergonomic approach. This is also adjacent to the ergonomic definition of FS as such a state of the human body, which is assessed according to the results of labor and professional activity. And it is the results of such activities that are considered as the most integral indicator of the functional state. At the same time, a decrease in the effectiveness of activities is considered as a sign of deterioration of the FS.
In the first case, it means “operational rest” - a special state of readiness for an activity in which the human body is capable of turning into various forms of physiological activity for a specific activity in a short period of time. The state of operative rest is accompanied by an increase in the tone of the nerve centers, especially those that are related to the construction of movements associated with the intended labor actions and operations, as well as the stress of some vegetative functions.
In the second case, we are talking about the so-called extreme states (reactive borderline or pathological states).
Of course, between the state of operational rest and extreme states, there are quite a few other states of the type: fatigue, thermal stress, water depletion, etc.
This method of assessing the FS is certainly useful in solving problems of improving the efficiency of labor. In addition, it allows you to predict the development of unwanted FS such as monotony, stress, or a high degree of fatigue. However, as mentioned above, this approach does not allow to approach the solution of the problem of the mechanisms of formation and change of FS.
The psychophysiological approach to determining functional states is based on the idea of the existence of modulating systems of the brain. According to this approach, the emphasis is on the functional specialization of the two body systems.
Both modulating systems, being closely connected with the higher parts of the cerebral cortex, form a special functional system that has several levels of response: physiological, behavioral, psychological (subjective). In accordance with this logic, the functional state can be considered as the result of the activity of the combined functional system.
Thus, in psychophysiology, the functional state acts as the result of the interaction of the modulating systems of the brain and the higher parts of the cerebral cortex, which determines the current form of the individual's life activity.
This definition gives grounds to draw the line between different functional states not only by behavioral manifestations, activity efficiency or the results of polygraphic registration, but also by the level of activity of the modulating systems of the brain.
The level of wakefulness is an external manifestation of the activity of the nerve centers. This concept characterizes the intensity of behavior. All behavioral manifestations in the first approximation can be considered as a continuum (or one-dimensional scale), due to fluctuations in the excitation of modulating systems of the brain. According to some ideas, there is a continuous series of changes in the level of wakefulness between sleep and the state of extreme arousal, caused by changes in the activity levels of the nerve centers. Maximum efficiency of activity corresponds to the optimal level of wakefulness.
So, presumably changes in the functioning of nerve processes form a one-dimensional scale, the lower limit of which is the sleep state, the upper one - the state of very strong excitement such as rage. It is assumed that between these poles there are a number of levels of wakefulness that make up the range of intensity of behavior. Changes in the levels of wakefulness cause changes in the tone of the nerve centers: every nervous activation must be expressed in increased wakefulness.
The scheme describing the linear continuum of levels of wakefulness, however, requires two important clarifications.
Firstly , it has been established that the activity of the nerve centers during sleep is not always minimal. As will be shown below, during some periods of a night's sleep, the human body detects the stress of physiological functions. Probably, it should be recognized that there are qualitative differences between different FSs, which cannot be reduced only to differences in activation levels.
Secondly , the idea of a consistent increase in levels of wakefulness does not imply that the adaptive abilities of the organism also increase monotonously. Starting from a fairly high level of wakefulness, most of the actions are disturbed, thus the effectiveness of the activity performed is related to the level of wakefulness by inverse U-shaped dependence. Theoretically, it can be assumed that for each type of adaptive behavior there is an optimal level of wakefulness.
Thus, it is necessary to introduce the concept of the optimum level of wakefulness and the corresponding functional state, against which a person achieves the highest results. It should be noted that there is no quantitative measure for fixing the level of wakefulness, i.e. one cannot directly measure the level of wakefulness, such as measuring body temperature. The transition from one level of wakefulness to another is estimated empirically, on the basis of observation and quantitative assessment of various physiological parameters.
The neurochemical approach to the determination of functional states is based on the idea of a strong dependence of the mental state of a person (his moods and experiences) on the biochemical composition of the internal environment of the body. It is assumed that in the human brain there is a special mechanism that regulates the functional state through a change in the level of activity of the mediator systems of the brain, as well as the balance of their activity (Danilova, 1992). Stable equilibrium activity of mediator systems gives an idea of the average level of activation or functional state at which this behavior is realized. Different types of behavior correspond to different balances in the activity of the mediator systems of the brain.
Changes in the levels of wakefulness are associated with changes in the tone of the corresponding nerve centers, and several levels of regulation of wakefulness can be distinguished: cellular, individual centers, and the brain as a whole.
Neural mechanisms. At the neural level, the regulation of functional states is carried out with the help of a special category of neurons, called modulatory. There are two categories of modulatory neurons: the activating and inactivating types. The former increase the activity of synapses connecting sensitive and executive neurons, the latter decrease the effectiveness of synapses, interrupting the transmission of information from afferent to efferent neurons. In addition, modulating neurons differ in the degree of generalization of their actions. Transition to an unconscious state, for example, when falling asleep, can be defined as turning off activating neurons-modulators of a generalized type and turning on inactivating neurons-modulators.
In evolution, neuron-modulators united in ensembles and networks, concentrated at the level of the reticular formation of the brain stem and the nonspecific thalamus, forming an activating and inactivating system.
Modulating systems. The combination of modulating systems forms a special block that regulates the tone of the cortex and subcortical structures, optimizes the level of wakefulness in relation to the activities performed and causes an adequate choice of behavior in accordance with the actualized need.
The most important part of the regulatory block is the reticular formation of the brain, representing a network of nerve cells in the middle of the trunk. On the sides, the reticular formation is surrounded by sensory pathways, which give a part of afferent impulses to the reticular formation. Due to this, any sensory stimulation increases the level of activation of the reticular formation, activation along the ascending paths extends upward to the cortex of the big hemispheres. It was experimentally shown that stimulation of the reticular formation through electrodes implanted into it leads to the awakening of a sleeping animal.
Another important link in the regulation of functional states is associated with the work of the thalamus. The visual hillock, or thalamus, is a section of the diencephalon, which acts as a collector of sensory information, since it receives information from all the sense organs. According to some information, in the center of the thalamus there is a “pacemaker” - a morpho-functional formation responsible for the generation of rhythmic activity and spreading synchronized effects on vast areas of the cortex. The nuclei of the non-specific thalamus form a diffuse projection thalamic system, which has stimulating and inhibitory effects on the cortex. These effects are more limited compared to the effects of brain stem excitation and capture relatively small areas of the cortex.
Thus, during stimulation of the thalamus, an activation reaction occurs in the cerebral cortex. This reaction is clearly visible in the current electroencephalogram: it is relatively short-lived and localized. In contrast to the activation reaction caused by the reticular formation of the brain stem, which is considered a generalized activation reaction, the effects of the excitation of a nonspecific thalamus are called local activation.
Table 3.1. The main differences in the effects of brain stem and thalamus activation
| Reaction characteristics | EEG trunk activation | EEG activation of the thalamus |
| Distribution area | Generalized | Local |
| Reaction type | Tonic | Phasic |
| Temporal dynamics | Slowly fading away | Fast fading |
Consequently, the transfer of the relay of activating influences from the level of the reticular formation of the brain stem to the level of the thalamic system means a transition from generalized activation of the cortex to the local one. The first is responsible for global shifts of the general level of wakefulness. The second is responsible for the selective, i.e. selective focusing (see topic 6, paragraph 6.3).
Another modulating system of the brain, the limbic system of the brain with activating and inactivating divisions, takes part in regulating the level of wakefulness and ensuring selective modulation and actualization of a particular need (see Topic 4, Section 4.2).
Regulation of functional states at the level of the whole brain. The most important regulator of the level of wakefulness in general and attention as an electoral process are the anterior sections of the cerebral cortex - the frontal zones. It is these structures that, in the descending cortico-reticular pathways, modulate the activity of the stem and thalamic systems in the right direction. The inclusion of frontal zones into this process with their descending paths suggests the existence of a kind of closed control loop. Initially, the reticular formation of the brainstem, excited by external stimuli, activates the nonspecific thalamus and cortex of the cerebral hemispheres, and that, in turn, due to the descending pathways, can reduce the activity of the reticular formation of the trunk and thalamus or increase depending on what is required at the moment of time. Thus, it is possible to speak about the existence of a regulated or controlled cortical activation, due to which the cerebral cortex can adjust its own level of excitability according to the tasks of the current life activity.
Physiological methods for diagnosing functional states are a special class of methods and indicators by which one can reliably and objectively judge the current state of the body and its changes. A detailed analysis of methods of psychophysiology was presented in the appropriate section (see topic 2). Consider the specifics of their use in the diagnosis of functional states.
EEG indicators of FS. Changes in the parameters of the electrical activity of the brain are traditionally used as a direct indicator of the dynamics of the level of activation. Characteristic changes in the spectral composition of the EEG correspond to different levels of wakefulness. For calm wakefulness, the prevalence of the alpha rhythm is typical, the severity of which increases even more with closed eyes. When you open your eyes and increase the level of wakefulness, the blockade of the alpha rhythm occurs. The active wakefulness is characterized by desynchronized EEG with the predominance of high-frequency components of beta and gamma rhythms. With emotional stress and mental activity in the EEG, the theta rhythm may appear and intensify. In a state of fatigue, slow-wave activity in theta and delta bands begins to appear more clearly. As fatigue increases, the duration of these periods increases and a picture of “hypersynchronization” of the EEG appears. The delta rhythm is also most characteristic for a particular stage of sleep (see section 3.2).
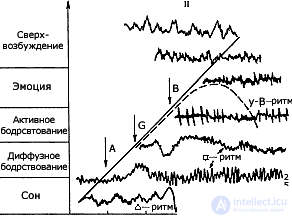 The dynamics of the EEG depending on the levels of wakefulness (according to V. Blok, 1970):
The dynamics of the EEG depending on the levels of wakefulness (according to V. Blok, 1970):
I - levels of wakefulness; II - EEG rhythm dynamics at different levels of wakefulness; And - awakening from a dream; B - the awakening of attention; In - the awakening of emotions. A straight line indicates an increase in wakefulness levels within the continuum. The dotted line indicates the dynamics of the effectiveness of activities depending on the level of wakefulness.
The spatio-temporal organization of the brain's bioelectrical activity and its dynamics are closely related to the peculiarities of the functional state of the brain, therefore along with the assessment of individual rhythmic components of the EEG, the characteristics of their spatial-temporal relations, in particular, the indicators of coherence are used (see topic 2). The average level of coherence can be determined for individual frequency ranges (for example, alpha or beta) and for two power spectra over all frequencies taken together. It is established that the average level of coherence, calculated for symmetric points in different hemispheres or for two points in one hemisphere, with a constant functional state, is individually stable and retains its value after several days and months. A good indicator of the normal state of the brain is also the average level of coherence for the individual spectral components (delta, theta, alpha and beta).
Changes in FS in a healthy person, as a rule, are accompanied by restructuring of the spatio-temporal ratios of the brain biocurrents, while the connections between individual brain regions or spectral components can weaken, while others increase. However, as the correlation analysis shows, with a general mobilization readiness or with an increase in the complexity of the task being carried out, the intensity of most interregional ties may increase.
Dynamics of vegetative indicators. In the diagnosis of functional states, indicators of the cardiovascular, muscular, respiratory, excretory, and other body systems are successfully used.
For example, the heart rate, the strength of the heart contractions, the minute volume of the heart, the blood pressure, the regional blood flow naturally change with changes in functional states, primarily against the background of great physical exertion. With intensive work, the minute volume can increase almost tenfold: from 3-5 liters to 25-30 liters, the heart rate and blood flow in skeletal muscles increase significantly, and blood pressure can increase.
However, in the absence of physical exertion, changes in the same indicators are ambiguous. In other words, with the same external stimuli, opposite changes in the indices of the cardiovascular system can be observed. These facts have their own natural explanation.
The regulation of hemodynamics (stroke and minute blood volume, blood pressure, blood distribution throughout the body) is carried out with the help of the sympathetic and parasympathetic divisions of the nervous system. Both sections, in turn, are under the control of the highest vegetative center of the body - the hypothalamus and a number of other subcortical structures. Therefore, changes in the state of the sympathetic and parasympathetic divisions are systemic, i.e. naturally manifested in the state of most organs and systems.
The following are some specific reactions for which the sympathetic and parasympathetic systems are responsible:
Table 3.2. Effects of the Sympathetic and Parasympathetic Systems
| Systems and organs | Sympathetic system | Parasympathetic system |
|---|---|---|
| Pupil | Expansion | Constriction |
| Lacrimal gland | - | Secretion enhancement |
| Salivary glands | Small amount of thick secret | Bountiful Watery Secret |
| Heartbeat | Gain | Quit |
| Heart contractility | Gain | Quit |
| Blood vessels | Overall narrowing | Weak influence |
| Skeletal muscle | Toning up | Relaxation |
| Breathing rate | Gain | Quit |
| Bronchi | Lumen dilation | Narrowing of the lumen |
| Sweat glands | Activation | - |
| Adrenal glands and medulla | Adrenaline and norepinephrine secretion | - |
| Sex organs | Ejaculation | Erection |
| Gastrointestinal motility and tone | Braking | Activation |
| Sphincters | Activation | Relaxation |
Thus, with the predominance of excitation of the sympathetic nervous system, there will be one variant of the vegetative response, and with the initiation of the parasympathetic one, the other will be present. The sympathetic nervous system is designed to ensure the mobilization of the organism to activity, therefore, the state of mobilization and action will proceed against the background of vegetative changes according to the sympathetic variant. With a decrease in the level of tension and calm, the tone of the sympathetic nervous system will decrease and the parasympathetic tone will increase, while all changes in the body systems will have a corresponding dynamics. For the diagnosis of these autonomic changes can be used all the specific teaching methods described in topic 2.
Cyclicity is inherent in many phenomena in the surrounding world. We are accustomed to the rhythmic change of day and night, seasons, work and leisure. Biological rhythms, primarily the so-called circadian rhythms, caused by the rotation of the Earth around its axis, are of great importance for all living things.
Types of sleep. In humans and many animals, the period of sleep and wakefulness is timed to a daily change of day and night. Such a dream is called monophasic. If the change of sleep and wakefulness occurs several times a day, sleep is called polyphasic. Periodic daily sleep of an adult, as a rule, is monophasic, sometimes phase-wise (twice a day), a young child has a polyphasic type of sleep.
Seasonal sleep (hibernation) is also observed in a number of animals due to unfavorable environmental conditions for the body: cold, drought, etc.
In addition to these, several other types of sleep are described: narcotic (caused by various chemical or physical agents), hypnotic and pathological . The last three types of sleep are usually considered as a consequence of the non-physiological effects on the human or animal body.
Drug sleep can be caused by various kinds of chemical effects: inhalation of ether vapor, chloroform, the introduction into the body of various kinds of drugs, such as alcohol, morphine and others. In addition, this dream can be caused by electroneurosis (the impact of an intermittent electric current of weak force).
Pathological sleep occurs when anemia of the brain, brain injury, the presence of tumors in the cerebral hemispheres or damage to some parts of the brainstem. This also includes lethargy, which can occur as a reaction to a strong emotional trauma and can last from several days to several years. The phenomenon of pathological sleep should also include sleepwalking (somnambulism), the physiological mechanisms of which are still unknown.
Of particular interest is hypnotic sleep , which can be caused by the hypnotic effect of the setting and the effects of the hypnotist. During hypnotic sleep, it is possible to turn off arbitrary cortical activity while maintaining partial contact with others and the presence of sensorimotor activity.
The alternation of sleep and wakefulness is observed at all stages of the evolutionary ladder: from lower vertebrates and birds to mammals and humans. There is no doubt that such a universal organization of rhythmic alternation of activity and rest has a deep physiological meaning. It is well known that during sleep significant physiological changes occur in the work of the central nervous system, the autonomic nervous system and other systems and functions of the body.
Among the basic laws of human mental activity is the cyclical alternation of sleep and wakefulness.
However, it should be noted, and frequent violations of the rhythm of sleep, which include insomnia and the so-called insurmountable sleep (narcolepsy) that occurs during passive driving, when performing monotonous work, as well as when driving various vehicles: car, electric locomotive, metro.
Sleep stages Man's sleep has the right cyclical organization. During sleep, there are five stages. Four stages of slow-wave sleep and one stage of rapid. It is sometimes said that sleep consists of two phases: slow and fast. The completed cycle is considered to be a segment of sleep, in which there is a successive change of the stages of slow-wave sleep with fast sleep. On average, there are 4-6 such cycles per night, lasting about 1.5 hours each.
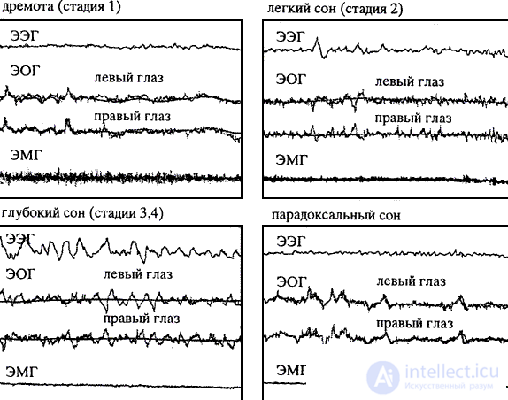 Fragments of a polygram at different stages of sleep (according to VM Kovalzon, 1999).
Fragments of a polygram at different stages of sleep (according to VM Kovalzon, 1999).
It can be seen that a gradual increase in amplitude and a decrease in the frequency of EEG waves, a change in fast eye movements with slow ones, up to complete disappearance, are characteristic of changing the stages of slow sleep; progressive decrease in the amplitude of the EMG. When paradoxical sleep, EEG is the same as when awake, EOG demonstrates rapid eye movements, and EMG is almost not recorded
In-depth study of sleep was possible only after the invention of electroencephalography. It was with the help of EEG that significant differences were found both between the stages of sleep and between the state of sleep and wakefulness.
The first stage is transitional from waking state to sleep, which is accompanied by a decrease in alpha activity and the appearance of low-amplitude slow theta and delta waves. The duration of the first stage is usually not more than 10-15 minutes. At the end of this stage, short flashes of so-called sleep spindles may appear, clearly visible against the background of slow-wave activity. However, until the sleep spindle reaches a duration of 0.5 seconds, this period is considered the first stage of sleep. In the behavior of this stage corresponds to the period of drowsiness with half-awake dreams, it can be associated with the birth of intuitive ideas that contribute to the success of solving a particular problem. The second stage takes a little less than half of all night sleep. This stage is called the stage "sleep spindles", because its most prominent feature is the presence in the EEG of a spindle-shaped rhythmic activity with a frequency of 12-16 Hz. The duration of these “spindles”, which stand out well from the background high-amplitude EEG with a mixed frequency of oscillations, ranges from 0.2 to 0.5 seconds.
The third stage is characterized by all the features of the second stage, to which is added the presence in the EEG of slow delta oscillations with a frequency of 2 Hz or less, occupying from 20 to 50% of the recording era. This transitional period lasts only a few minutes.
The fourth stage is characterized by the predominance of slow delta oscillations with a frequency of 2 Hz or less in the EEG, which occupy more than 50% of the epoch of night sleep. The third and fourth stages are usually combined under the name of delta sleep. The deep stages of delta sleep are more pronounced at the beginning and gradually decrease towards the end of sleep. In this stage, waking up a person is quite difficult. It is at this time that about 80% of dreams occur, and it is at this stage that sleepwalking and nightmares are possible, but the person remembers almost none of this. The first four stages of sleep normally occupy 75-80% of the entire sleep period.
The fifth stage of sleep. The fifth stage of sleep has a number of names: the stage of "rapid eye movements" or abbreviated BDG, "fast sleep", "paradoxical sleep". During this stage, a person is in complete immobility due to a sharp drop in muscle tone, and only eyeballs under close eyelids make fast movements with a frequency of 60-70 times per second. The number of such movements can vary from 5 to 50. Moreover, a clear connection was found between rapid eye movements and dreams. So, in healthy people, these movements are larger than in patients with sleep disorders. It is characteristic that people who are blind from birth dream only of sounds and sensations. Their eyes are motionless. It is believed that the intensity of BDG can be judged on the brightness and emotionality of dreams. However, eye movements in a dream are different from those that are typical for viewing objects in the waking state.
In addition, at this stage of sleep, the electroencephalogram acquires signs characteristic of the waking state (low-amplitude high-frequency components prevail in the spectrum). The name "paradoxical" arose because of the apparent discrepancy between the state of the body (complete rest) and brain activity. If at this time to wake the sleeper, then in about 90% of cases you can hear the story of a vivid dream, and the accuracy of the details will be significantly higher than when you wake up from a slow sleep (see. Fig. Mirror galvanometer).
The paradoxical stage of sleep is present in many species of mammals and even in some species of birds. It is also noted that in animals the proportion of paradoxical sleep tends to increase with an increase in the degree of development of the cortex. However, paradoxical sleep in animals and humans takes place in different ways. A man in a paradoxical dream is motionless (only his eyes move). In animals, whiskers, ears, and tails move, paws twitch, blinkers and sucking movements occur, and even squeals are heard in dogs.
Sleep BDG periods occur at approximately 90 minute intervals and last an average of about 20 minutes. In normal adults, this stage of sleep takes about 20-25% of the time spent in sleep. In infants, this proportion is much higher; in the first weeks of life, about 80% of the very long sleep time is paradoxical sleep.
The need for sleep. This vital need depends on age. So the total duration of sleep for newborns is 20-23 hours a day, at the age of 6 months to 1 year - about 18 hours, at the age of 2 to 4 years old - about 16 hours, at the age of 4 to 8 years - 12 hours; at the age of 8 to 12 years old - 10 hours; at the age of 12 to 16 years old - 9 hours. Adults sleep on average 7-8 hours a day.
Argued that the need for sleep to old age is reduced.
However, it has been established that people over 60, suffering from various diseases, sleep, as a rule, for less than 7 hours a day. At the same time, practically healthy people of this age sleep more than 8 hours a day. With an increase in the duration of sleep in "low-sleeping" elderly people, an improvement in their state of health is observed. According to some data, the duration of sleep of the long-livers of the Caucasus varies from 9 to 16-17 hours per day. On average, long-livers sleep for 11-13 hours. In other words, as a person ages, the duration of sleep should increase.
Sleep-deprived person dies within two weeks. Sleep deprivation for 3-5 days causes an overwhelming need for sleep. As a result of a 60-80 hour lack of sleep, a person experiences a decrease in the rate of mental reactions, mood deteriorates, disorientation occurs in the environment, performance decreases dramatically, rapid fatigue occurs during mental work and less accuracy. A person loses the ability to focus attention, there may be various disorders of motility (tremor and tics), and hallucinations are possible, sometimes there is a sudden loss of memory and confusion of speech. With longer sleep deprivation, psychopathies and even paranoid mental disorders can occur.
Changes in vegetative functions during prolonged insomnia are very small, there is only a slight decrease in body temperature and a slight slowdown in the pulse.
The science describes several cases of prolonged lack of sleep, which, along with the phenomena of somnambulism (sleepwalking) and lethargic sleep, have not yet been explained. Most often, these cases were associated with strong mental shocks (loss of a loved one, consequences of a catastrophe). However, in most cases, such events lead to the opposite result - to lethargic sleep.
Slow and paradoxical sleep is equally necessary for the body. So, if you wake a person every time a paradoxical dream occurs, the tendency to fall into a paradoxical dream will increase. After a few days, the person will move from wakefulness to paradoxical sleep without an intermediate phase of normal sleep.
Thus, the stages of sleep form a kind of system in which the impact on one link entails a change in the state of the other link.
Physiological changes during sleep. The most characteristic symptoms of sleep include a decrease in the activity of the nervous system and the cessation of contact with the environment due to the "turning off" of the sensorimotor sphere.
Thresholds of all types of sensitivity (sight, hearing, taste, smell and touch) in a dream increase. The magnitude of the threshold can be judged on the depth of sleep. In the first four stages, thresholds of perception increase by 30-40%, while in BDG sleep - by 400%. Reflex function during sleep dramatically weakened. Conditioned reflexes inhibited, unconditioned significantly reduced. However, some types of cortical activity and reactions to certain stimuli can persist during normal periodic sleep. For example, a sleeping mother hears the sounds of the movements of a sick child. This phenomenon is called partial wakefulness.
Most of the muscles in a dream are in a relaxed state, and the person is able to maintain a certain posture of the body for a long time. At the same time, the tonus of the muscles covering the eyelids and the annular muscle locking the bladder are enhanced. As we sink into sleep, the rhythms of the heart and respiration slow down, becoming more and more uniform.
Slow-wave sleep is accompanied by a decrease in vegetative tonus - pupils narrow, the skin becomes pink, sweating increases, salivation decreases, cardiovascular, respiratory, digestive and excretory systems decrease, circulating blood volume decreases; there is excessive blood filling of the pulmonary vessels; respiratory rate decreases, which leads to restriction of the amount of oxygen entering the blood and slower removal of carbon dioxide, i.e. decreases the intensity of pulmonary gas exchange. That is why at night the heart rate decreases, and with it the speed of blood flow.
It should be emphasized that, although, in general, the level of metabolism decreases in a dream, at the same time the processes of restoring the health of all the cells of the body are activated, their reproduction is intensive, and proteins are replaced.
In contrast, during the paradox of sleep comes the "vegetative storm". Breathing becomes irregular, irregular, changing in depth. Possible and stop breathing (for example, in a nightmare). In men at this stage, there is an erection of the penis, which occurs not only in adults, but also in infants.
Throughout the night, the person activates the growth of hair and nails. The temperature of the human body during sleep decreases (in women it drops to 35.6 and in men to 34.9 degrees). Similar daily fluctuations in temperature — a decrease in the night and an increase in the afternoon — are also observed in the absence of sleep or during daytime sleep and night wakefulness.
With some forms of the so-called hypnotic sleep, and in particular with catalepsy ( catalepsy is the freezing of a person in his posture, sometimes very uncomfortable, requiring significant muscle tension ), a sharp increase in muscle tone occurs (see Chrestomat. 3.5).
The first ideas about the origin of sleep are mainly of historical interest. Thus, in accordance with hemodynamic theory, sleep occurs as a result of stagnation of blood in the brain in the horizontal position of the body. According to another version, sleep is the result of brain anemia and at the same time its rest. According to the histological theory, sleep occurs as a result of disruption of the connections between nerve cells and their processes, arising from the prolonged excitation of the nervous system.
Chemical theory According to this theory, during wakefulness, easily oxidized products accumulate in the cells of the body, resulting in an oxygen deficiency, and the person falls asleep. According to the psychiatrist E.Klapareda, we fall asleep not from being poisoned or tired, but in order not to poison ourselves and not be tired.
A histological analysis of the brains of dogs killed after ten days without sleep shows changes in the shape of the nuclei of the pyramidal neurons of the frontal cortex. At the same time, the blood vessels of the brain are surrounded by leukocytes and in some places are broken. However, if the dogs are given a little sleep before killing, no changes are detected in the cages.
According to some assumptions, these changes are caused by a special poison hypnotoxin. A compound prepared from blood, cerebrospinal fluid, or an extract of the substance of the brain of dogs that have not been sleeping for a long time was injected into awake dogs. The latter immediately found all signs of fatigue and fell into a deep sleep. The same changes appeared in their nerve cells as in dogs that had not slept for a long time. However, it was not possible to isolate hypnotoxin in its pure form. Moreover, PK’s observations contradict this theory. Anokhin over two pairs of Siamese twins with a common circulatory system - he very often observed that one head was sleeping, while the other was awake. If sleep is caused by blood-borne substances, the twins should fall asleep at the same time. However, it is not.
Chemical theory cannot also answer a series of questions.
For example, why does daily food poisoning do no harm to the body? Where do poisons go for insomnia? Why does a newborn baby sleep almost all the time?
Sleep like inhibition. According to I.P. Pavlov, sleep and internal inhibition in their physico-chemical nature are a single process. The difference between them lies in the fact that internal inhibition in a waking person covers only separate groups of cells, while in the development of sleep, inhibition widely radiates along the cortex of the big hemispheres, spreading to the lower parts of the brain. Such diffuse inhibition of the cortex and subcortical centers ensures their restoration for subsequent activity. Sleep, developing under the influence of inhibitory conditioned stimuli, I.P. Pavlov called active, opposing to him passive sleep, arising in the event of the termination or abrupt restriction of the influx of afferent impulses into the cerebral cortex.
Modern theories of sleep. Currently, most of the existing hypotheses regarding the functional purpose of sleep and its individual stages can be reduced to three main types: 1) energy, or compensatory-restoration, 2) information, 3) psychodynamic.
According to "energy" theories, during sleep, the energy expended during wakefulness is restored. A special role is given to the delta-sleep, the increase in the duration of which follows the physical and mental stress. Any load is compensated by an increase in the share of delta sleep. It is at the stage of delta sleep that the secretion of neurohormones occurs, which have an anabolic effect.
Selected morphological formations related to the regulation of sleep.
The reticular formation controls the initial stage of sleep. The hypnotic zone located in the anterior part of the hypothalamus also has a regulating effect on the functions of sleep and wakefulness. Peripheral hypnogenic zones are located in the walls of the carotid arteries. So, in the body there are a number of hypnogenic zones. The mechanism of the onset of sleep and waking from sleep is complex and probably has a certain hierarchy.
Theory P.K. Anokhin attaches importance to the functions of the hypothalamus in this process. With prolonged wakefulness, the level of vital activity of the cells of the cerebral cortex decreases, so their inhibitory effect on the hypothalamus weakens, which allows the hypothalamus to "turn off" the activating effect of the reticular formation. With a decrease in the upward flow of arousal, a person falls asleep.
Information theories claim that sleep is the result of a decrease in sensory flow to the reticular formation. The latter entails the inclusion of brake structures. Such a point of view was also expressed that not cells, not tissues, not organs, but mental functions: perception, consciousness, memory, need rest. Perceived information can "overflow" the brain, so it needs to disconnect from the surrounding world (which is the essence of sleep) and switch to another mode of operation. Sleep is interrupted when information is recorded and the body is ready for new impressions.
In one of the variants, the concept of synchronization in the work of brain structures is decisive. When fatigue synchronization is broken. As a result of disruption of biorhythm synchronism, a person feels tired. The benchmark for creating optimal consistency of rhythms is the “model of the required biorhythmic background,” which is created during wakefulness on the basis of an innate program of behavior and signals coming from outside.
To create a model you need external information. The more it gets the body, the less (despite the information theory) he will need sleep. In dreams, perhaps, this process of readjustment and streamlining of phase relations between structures is reflected. Then in a quick dream a kind of neuron training takes place; cells that were not involved in the affairs of the past day, in order not to "lose their shape", are forced to engage in functional gymnastics. Not without reason, after a strong shock, when every single neuron received a strong shake, a person sleeps like a dead man and does not dream of anything. He who leads a languid, devoid of life life, sees many dreams.
According to the famous neuropsychiatrist A.M. Wein, information theory does not contradict the energy concept of recovery, because the processing of information in a dream does not replace the processing during wakefulness, but complements it. Восстановление в самом широком значении этого слова — это не покой и пассивное накопление ресурсов, вернее не только покой, которого у нас во сне достаточно, но, прежде всего, своеобразная мозговая деятельность, направленная на реорганизацию воспринятой информации. После такой реорганизации и возникает у нас ощущение отдыха, физической и умственной свежести.
According to "psychodynamic" theories of sleep, the cerebral cortex has a inhibitory effect on itself and subcortical structures.
Psychodynamic theories include the homeostatic theory of sleep. In this case, homeostasis is understood as the whole complex of processes and states on which the optimal work of the brain is based. According to his theory, there are two types of wakefulness - calm and tense.
The calm is maintained by the activity of the reticulo-talamocortical system (activating the impulses that the reticular formation sends, induce the thalamus and the cerebral cortex to work more intensively), and stress, moreover, by the activity of the limbic system.
The combination of the work of these two systems provides intense wakefulness - the necessary basis for targeted and coordinated reactions. During REM sleep, one limbic system works: emotions are agitated, and coordinated reactions are paralyzed. Judging by the activity of brain structures, then fast sleep is an analogue of not calm, but intense wakefulness. The activity of the brain structures in quiet wakefulness and in slow sleep is different.
Many hypotheses have been put forward about the meaning of paradoxical sleep.
A number of researchers believe that these are periods of cell recovery, others believe that BDG sleep plays the role of a "safety valve" that allows the excess energy to be discharged while the body is completely motionless; according to the third opinion, the BDG dream helps to fix the information obtained during wakefulness in memory. Some studies even point to the close relationship between high levels of intellectual development and the large total duration of periods of paradoxical sleep in many people.
REM sleep itself can be divided into two stages. Against the background of continuous desynchronization, which lasts from 5 to 20 seconds and is accompanied by rapid eye movements, the theta rhythm generated by the hippocampus is developing rapidly. This is the emotional stage of REM sleep. Then the theta rhythm weakens, and in the meantime the alpha rhythm, a sign of emotional indifference, increases in the new cortex, especially in its sensory-motor area. Then the alpha rhythm weakens, and in the hippocampus the theta rhythm increases again.
Both stages, emotional and non-emotional, alternate several times during sleep, the first is always longer than the second.
Strengthening of theta rhythm in fast sleep is accompanied by the same vegetative phenomena that accompany intense wakefulness, saturated with strong emotions. In both sleep and wakefulness, the hippocampal theta rhythm stems from the same source: this is a reflection of the powerful flow of impulses generated by the posterior hypothalamus, one of the most active participants in intense wakefulness. Both in a dream, and in wakefulness the same structures, the same rhythms, and obviously, the same emotions are involved. Only during sleep the muscles are relaxed and the mind is turned inward - that’s all the difference.
Conclusion According to some ideas, there is a hierarchically constructed brain system regulating the cycles of sleep and wakefulness. The reticular activating system, which maintains the level of wakefulness, the synchronizing apparatuses responsible for slow sleep and the reticular nuclei of the pons, responsible for fast sleep, are included in the regulated contour of this system. In the control loop, the interaction between these devices, their inclusion and change. In the same place, sleep and wakefulness are connected with other systems of the body - vegetative, somatic, mental. There is no doubt that the regulatory circuit is located within the limbico-reticular complex. Inside this complex there are also specialized devices (vasomotor and respiratory centers, hypothalamus nuclei regulating the activity of the pituitary gland and amplifying shifts in the internal environment, zones providing sleep and wakefulness) and neural formations that integrate the activity of the brain systems.
 Stress is often considered as a special functional state and at the same time as a psycho-physiological response of the body to environmental influences that go beyond the limits of the adaptive norm. The term "stress" was introduced by Hans Selye in 1929. As a medical student, he drew attention to the fact that all patients suffering from various diseases, a number of common symptoms (loss of appetite, muscle weakness, high blood pressure and temperature, loss of achievement motivation). Since these symptoms do not depend on the nature of the somatic disorder, Selye proposed to designate such a condition as “just a disease syndrome”. Originally Selye used the term "stress" to describe the totality of all nonspecific changes (inside the body), functional or organic. One of the latest definitions of stress is: “a non-specific response of an organism to any demand from outside” (Selje, 1974).
Stress is often considered as a special functional state and at the same time as a psycho-physiological response of the body to environmental influences that go beyond the limits of the adaptive norm. The term "stress" was introduced by Hans Selye in 1929. As a medical student, he drew attention to the fact that all patients suffering from various diseases, a number of common symptoms (loss of appetite, muscle weakness, high blood pressure and temperature, loss of achievement motivation). Since these symptoms do not depend on the nature of the somatic disorder, Selye proposed to designate such a condition as “just a disease syndrome”. Originally Selye used the term "stress" to describe the totality of all nonspecific changes (inside the body), functional or organic. One of the latest definitions of stress is: “a non-specific response of an organism to any demand from outside” (Selje, 1974).
Thus, in general, stress is a nonspecific component of adaptation, which plays a mobilizing role and leads to the attraction of energy and plastic resources for adaptive restructuring of the organism.
Types of stress. Selye believed that the stress response is a nonspecific set of psycho-physiological changes that does not depend on the nature of the stress-provoking factor. Later, however, it was shown that the overall picture of psychological reactions can be very specific. Both the qualitative originality of the stimulus and the individual characteristics of the organism contribute to its formation.
Due to the peculiarities of the stimulus, it is customary to distinguish at least two types of stress: physical (physiological, first-signal) and psychoemotional (second-signal).
The stress stimulus is called a stressor .
An irritant can become a stressor as a result of its cognitive interpretation, i.e. values that a person attributes to a given stimulus (psychoemotional stress). For example, the sound of someone else’s footsteps behind a person walking down the street at night in a deserted street can be a strong stressor. Physical stress arises as a result of exposure to a stimulus through a sensory or metabolic process. For example, asphyxiation or too much exercise take on the role of stressors that trigger physiological stress. The special role of the duration of exposure to an adverse factor should be emphasized. Thus, some stimuli can cause a stress reaction as a result of their rather long exposure to humans.
In the case of short-term stress, as a rule, already established response programs and resource mobilization are updated.
With prolonged exposure to stress factors, two options are possible.
In the first, there are restructuring of the functional systems responsible for mobilizing resources. And often these alterations can entail serious consequences for human health: for example, cardiovascular pathology, diseases of the gastrointestinal tract, etc.
In the second case, the restructuring of functional systems as such does not occur. In this case, reactions to external influences are predominantly local. For example, physical stimuli (extreme heat or cold, loud noise, stuffiness, etc.) act on the lower sensory mechanisms, and such stimuli as coffee, nicotine, various neuroleptics, etc. - act on the body through the digestive tract and metabolic processes.
Physiological stress is usually associated with an objective change in the conditions of human life. In contrast, psychoemotional stress often occurs as a result of an individual's own position. A person reacts to what surrounds him, in accordance with his interpretation of external stimuli, which depends on personal characteristics, social status, role-playing behavior, etc. Applying caffeine, alcohol, nicotine, drugs, etc. to stress, a person only enhances the negative effects of stress.
The value of stress. The essence of the reaction to the stressor is the activation of all body systems necessary to overcome the "obstacle" and return the body to normal conditions of existence. If the stress response performs this function, its adaptive value becomes apparent. There is no doubt that adaptation is a biological function of stress. In this regard, stress is designed to protect the body from the threatening and destructive effects of various modalities, both mental and physical. Therefore, the occurrence of stress means that a person is involved in a certain activity aimed at confronting dangerous influences. At the same time, a special functional state and a whole complex of various physiological and psychological reactions arise. Thus, stress is a normal phenomenon in a healthy body - a protective mechanism of the biological system.
What has been said above is certainly true for physiological stress. However, the stress reaction that occurs in a modern person under psychoemotional stress can often be qualified as inadequate arousal of primitive defense mechanisms when the body is activated for physical activity (fight or flight). Under conditions of social regulation of behavior, there is no place for either one or the other. It is obvious that a civilized person cannot hit his opponent, even if he is absolutely sure that he is right.
The stress response that occurs repeatedly and does not receive discharge often leads to dysfunctional and pathological disorders characterized by structural changes in the tissue and the functional system of the target organ. When these changes are due to stress, this disease is called psychosomatic or psycho-physiological, a disease. Nevertheless, since the time of Selye, it is customary to distinguish between the constructive and destructive aspects of stress. In other words, not every stress is bad. Stress activation is often a positive force, enriching a person with an awareness of their real capabilities. Selye called positive stress eustress, and relaxing and destructive stress - distress. (By origin, the word "stress" means restriction or oppression, and the word "distress" means being in a state of restriction or oppression.)
At an early stage of development of stress, as a rule, the general state of health and state of health improves. However, continuing to grow, stress reaches its climax. This point can be called
продолжение следует...
Часть 1 3. PSYCHOPHYSIOLOGY OF FUNCTIONAL STATES
Часть 2 3.4. Pain and its physiological mechanisms - 3. PSYCHOPHYSIOLOGY OF

Comments
To leave a comment
Psychophysiology
Terms: Psychophysiology