Lecture
Although the simulation of a placebo effect in the laboratory allows one to demonstrate its phenomenology, this procedure remains rather isolated from the unfolded mythology of medicine. The results would be useful to supplement the “left” research included in the real therapeutic process. Such an opportunity was provided in 1987, when the author participated in the work of the Commission of the Cancer Research Center of the Russian Academy of Medical Sciences on the evaluation of the antitumor activity of the drug Catrex. The situation is as follows. In 1987, an article appeared in the magazine “Smena” stating that A.G. Gochichiladze invented a very effective anticancer drug, which showed brilliant results in testing, but was not put into practice because of the disinterest of the USSR Ministry of Health (Berdichevskaya, 1987). After the publication of the article, the situation became uncontrollable: tens of thousands of cancer patients and their relatives arrived in Georgia to receive the miraculous drug and the USSR Ministry of Health in several research institutions immediately conducted its clinical trials. Although trials showed the absence of any objective antitumor effect of the invented drug, this did not convince the author himself or his supporters. Their main argument was the obvious subjective efficacy of treatment with “catrex”, which allows it to be released to date.
|
|
The method itself met all the criteria of the classical healing myth: the possibility of the existence of a miraculous drug that cures cancer; persecuted and unrecognized author, surrounded by the ill will of colleagues; the drug itself was made from "natural raw materials" - the liver of a katran shark. Numerous publications and television programs have emphasized that sharks are the only species of living beings who do not have malignant tumors. In the spirit of
|
|
Mythopoetic thought suggested that the body of a shark contains some substance that, when extracted, can cure cancer and humans. In an emotionally charged atmosphere of oncology, myths of this kind are born with amazing regularity: the Troitskaya vaccine and the preparation AU-8, followed by oncological patients, traveled to Tallinn.
But this time the scale of events was not comparable with anything. Tens of thousands of people spent the night near the laboratory where KAT-REKS was produced, during the day the staff was busy working on it, and at night, at night fires, they gave it to those who waited. It was recommended to keep the ampoules stored in the refrigerator immediately before the administration, to warm the breath, and the treatment turned into a sacred act.
The situation of clinical trials was convenient for the study, as patients were under constant control; it was possible to observe in dynamics and an objective assessment of the therapeutic effect.
The hypothesis of the study: it was assumed that the subjective effect of treatment with “catrex” is determined solely by individual psychological factors (features of the cognitive style, elaboration of subjective intraceptive semantics, body language) and degree of assimilation of the myth underlying this treatment.
The main task of this block of research was to identify exactly what the subjective effect of treatment consisted of and what specific psychological factors determined its magnitude.
Chapter 9. The study of factors of subjective efficiency 221 9.2. Characteristics of patients
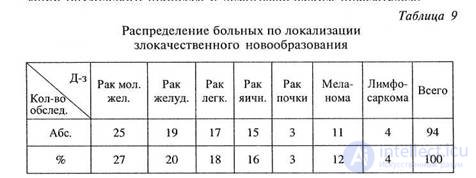
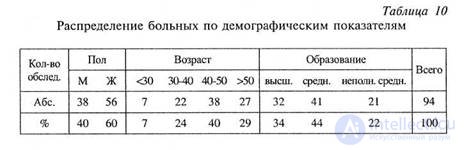
A total of 94 patients with various malignant neoplasms were examined in dynamics, 55 of which were able to carry out most of the studies and to follow in dynamics over 2 weeks. Tables 9 and 10 show the distribution of patients according to the localization of the tumor process and demographic indicators.
Patients were admitted to the clinic in various somatic conditions, some of them were able to be examined in full, the other part was so unfavorable that they had to be limited to clinical conversation.
The most important point of the study was the assessment of the subjective efficacy of the treatment. The main criterion was the opinion of the patient, which was clarified during the conversation. It became clear to the patient exactly what, in his opinion, was the effect of the treatment being carried out, how his well-being, complaints, objective manifestations of the disease had changed, what he expected from the treatment being carried out. As a result, all patients were divided into 2 groups: with the subjective effect of the treatment and without effect.
The first group included patients who for at least two weeks confidently noted the effect of treatment and could state what exactly it was.
The second group included patients who either did not notice any changes in their condition, or these changes were short-term and unstable.
Upon admission of patients to the clinic during the first conversation before treatment, the degree of patients' confidence in the expected effect was assessed. All patients were divided into three ranks of the degree of confidence in the effectiveness of treatment.
3 - patients who express unshakable confidence in the success of treatment with “catrex”, who believed that he “would definitely help them”. As a rule, this group included people who were well aware of the drug used, and turned on their own with the requirement to include them in a group of volunteers for clinical trials. Often, these people showed perseverance and perseverance in achieving their goals, attempted to independently get the drug and did not listen to the opinions of those who doubted the effectiveness of the “katrex”.
2 - patients who suggested that the “catrex” “could help” them, who believed that he was able to “activate the protective forces”. At the same time, their expectations were, as a rule, vague, the knowledge about the drug was fragmentary and the main role in including them in the test group was played by relatives rather than the patients themselves.
1 - patients who did not have a definite opinion on the possible effectiveness of treatment. Basically, this group included persons who were invited to participate in clinical trials by their attending physicians, or they were included in the group after learning about the trials by chance.
When planning an experiment, we tried as much as possible to maximize the set of parameters and methods studied, conducting a long survey that included various questionnaires: MMPI, Rotter locus control scale, measurement of the level of anxiety, etc. When processing the results, the informativity of the results obtained was evaluated in relation to the subjective effectiveness of treatment. Only two methods turned out to be highly informative.
A. The “hidden figures” test by G. Vitkin ( Witkin , 1954; Witkin et al., 1962; Soloviev, 1977; Witkin , Jooclenough , 1982).
This test, measuring the degree of “field addiction”, was developed within the framework of cognitive style research. The problem is that the subject must find simple geometric shapes that form part of a more complex pattern. Field-independent subjects easily perform this task, field-dependent people need a longer time. Initially, field dependence was understood as a function of perceptual differentiation: subject-dependent subjects perceived perceptual stimulation as a whole, hardly identifying its parts. In recent years, the interpretation of this phenomenon has become somewhat complicated. Field independence was understood as the subject's ability to focus on his own feelings, rather than on the context of stimulation presentation (coarsening is the choice of either his own body or perceptual field as a coordinate system). The essence of field dependence is easy to understand from the classical experiment of G. Vitkin “orientation of body position in space”. The subject is located in a small room, which can be tilted in different planes relative to the seat in it. Task: changing the position of the chair, give it a strictly horizontal position. Field-dependent subjects are guided not by their own proprioceptive sensations, but by the position of the room. A simpler test of “hidden figures” allows measurement of the degree of field dependence without complicated experimental equipment, by fixing the time spent searching for “hidden figures”.
B. The second very informative parameter turned out to be the degree of representation in the mind of bodily functions, as measured by the questionnaire “Body Perception Scale” (STI). According to the creators of this questionnaire, a person has not a level, inborn or acquired during ontogenesis, the level of “body perception” - the ability to be aware of vegetatively controlled body functions ( Main , 1983).
Strictly speaking, the questions included in this questionnaire relate not only and not so much to the vegetative nervous system, as to the totality of intraceptive sensations associated with the work of the internal organs: the heart, lungs, and the gastrointestinal tract. Normally, in a perfectly healthy person, these functions are performed, as a rule, automatically and are not recognized.
It is absolutely unimportant for us what is the true cause of an increase in the level of vegetative perception: somatic disease that violates the normal (and therefore unconscious) exercise of bodily functions, anxiety affecting the vegetative nervous system and through it objectified, innate vegetative talent, hypochondriacity or body experience. It is important that the assessment
patients with violations of bodily functions, in terms of their frequency or intensity, speak of at least two phenomena: their objectivity (representation in consciousness) and the development of the language of their description.
The subjective effect of treatment with “catrex” was observed in 62% of patients. Its value fluctuated somewhat over time, but on the whole it remained independent of the objective course of the disease.
Generally, improvements were noted, described as changes in the general state - “fatigue decreased,” “there was more strength”, or vegetative manifestations — decreased heartbeat, sweating, dizziness, temperature, shortness of breath. Very often, patients noted a decrease in pain, normalization of sleep, a decrease in anxiety. Some patients (34%) noted objective changes: reduction in the size or density of the tumor, swelling of the surrounding tissues, and ascites. The absence of objective changes in measuring them did not convince them at all, and in place of one unwarranted "improvement" another was chosen. Such improvements did not at all depend on the actual condition of the patients and were noted by them until death. One and the same symptom, depending on its interpretation, could be regarded as both positive and negative and, accordingly, experienced. In some patients, “katrex”, according to them, “normalized the temperature”, while others had a pyrogenic reaction that occurred after some injections was regarded as evidence of the effectiveness of treatment 1, and in the latter case the temperature rise itself was experienced as “pleasant”.
The condition of patients after injections changed so rapidly that it was impossible to explain these changes by the hypothetical activity of the drug. The nature of the changes themselves fully corresponded to the concept used. Supporters of "immunization" noted a "surge of strength," an improvement in the general condition, and those who
-1 It is interesting to compare this phenomenon with the results of the classical experiment of S. Schechter: 2 groups of students were examined in a hostile environment, and 2 others in a friendly relationship. One of each pair of groups received an injection of adrenaline, and the other injection of saline. The first group experienced negative emotions, and the second positive. The effect of adrenaline was unexpected. He amplified both positive and negative emotions. Whatever the physiological state of the injection, its sign was determined by the installation, and not by the substance ( Schacter , Singer , 1962).
He was guided by the “local effect”, assuming the presence of a certain active substance in the “catacre”, experienced localized sensations. One of the patients, drawing attention to the fact that the drug administered to her was “too transparent,” began to be suspected by the medical staff that they injected water, and her suspicions were fully confirmed by the “disappearance of the effect”. The smallest number of any sensations was observed in patients with an inaccurate concept of treatment.
At our request, the patients kept diaries of their condition and below is a fragment of one of them. Of particular interest in this case is that the patient herself was a doctor by education and she built her very qualified description according to the laws of the natural science genre.
Patient K.G.P., 38 years old, doctor.
Breast cancer, condition after oophorectomy, chemotherapy.
“Condition after ovariectomy and chemotherapy: weakness, dizziness, a sharp decline in performance, nausea, poor sleep, depression.
Status localis: the breast is enlarged, tense, insensitive, “alien”.
Pronounced premenstrual syndrome: headache, backache, fatigue, irritability. Tides are frequent (after 30-40 minutes) and are difficult to bear.
25. VIII .87. In the evening, the 1st injection of "catrex."
26. VIII. After the 2nd injection, after 1.5 hours, a sensation of mild pain, a pulling sensation appeared in the node.
After the 3rd injection, the sensation intensified: it seems that something is going on inside the knot, the sensation of some kind of movement, a constantly ongoing process. Improved sleep. For the first time I began to sleep without sleeping pills and woke up fresh and vigorous. Mood improved, appetite appeared, nausea, weakness disappeared.
After the 4th injection of “cutrex”, I walked without fatigue for 3 hours and walked up the stairs to the 4th floor without shortness of breath and tachycardia.
28. VIII. After the 5th injection, a visual enlargement of the breast in volume, a slight swelling of the skin of the subclavian area, pain in this area and pain in the axillary lymph node during movement and palpation appeared.
6th injection. Gradually, fatigue, headache, apathy, drowsiness.
7th injection. Loss throughout the body, more in the bones of the pelvis, given in the legs, severe pain in the chest, subclavian area, chills, temperature is normal. The reaction should be regarded as similar to bacterial shock. After taking tavegil, calcium chloride and hot tea, the chill passed.
29. VIII. 8th and 9th injections. Soreness is preserved throughout the body, but somewhat less; breast tenderness, axillary lymph node increased, although visually the breast is much smaller in volume, softer: breast sensitivity has appeared. Chest "live", "own"; some local temperature rise.
10th injection. There is a slight ache in the back, there was pain under the left shoulder blade: constant, dull, aggravated by movement and deep breathing. Sharp painfulness of the l / node, limiting mobility of the right hand. Status localis: palpation of the breast is much smaller in size, softer.
31. VIII. 12th injection. The state of health is normal. Mild pain on palpation in the subclavian region. Status localis: the breast is completely soft, feeling that the swelling is concentrated only in a restricted area. On the skin of the lower segments (where edema was previously pronounced), a kind of emptiness was formed, causing an unusual feeling of lightness.
In parallel with all the changes, there is a feeling of movement, of some inner work in the body. Soreness of axillary lymph node remains.
I treat the onset of soreness as a positive thing: something like a transition of the process to an inflammatory response.
Performance increased, slept more calmly. Tides less often (in an hour), are transferred easier, pass faster.
3. IX. 18th injection. Reduction of pain in the axillary lymph node, the node became softer.
7. IX. In the evening she began the 2nd treatment with Katrex. Feeling good. Sleep returned to normal. More calm. Locally - without pronounced dynamics. Sensations of internal pressure in the chest are less pronounced, appear 1.5–2 hours after the injection and last for about 15 minutes.
Tides are even rarer, easier to flow. The state of the organism, on the structure and local manifestations stabilized.
15. IX. 42nd injection. The chest is soft, “light”, a small area of edema remains, the node is clearly contoured, and has decreased by approximately 1/3, by palpation, as compared with the original dimensions. The submagneal ganglion has become softer, the soreness is small, with palpation persists.
16. ix. 46th injection. Without dynamics.
17-22. Ix. Break in treatment.
17-20. Ix. Colds It is characteristic that for the entire rainy period, the acute respiratory disease was ill only 1 time, quite easily, and quickly returned to normal. She usually fell ill with the onset of rain and until the first snow she practically didn’t feel completely healthy.
20. IX.The axillary knot became painless. The rest is unchanged.
23. IX. 3rd course of treatment "katreksom."
23-26. Ix. Without visible dynamics.
29. IX. 60th injection. There is practically no edema. The tumor and axillary lymph node decreased almost before our eyes. Obviously, when administered 3 times, an optimal concentration of the drug is created. But at the same time, there was a heaviness behind the sternum, moderate tachycardia, which are stopped by taking valocordin: it is similar to myocardia as a result of intoxication. Thirst appeared, during the next days pain in the heart and tachycardia disappeared.
I believe that "Katrex" has a pronounced immunostimulating and anti-inflammatory effect. I expect from him exactly the kind of effect. Sometimes you need to give a slight push and the ability to fight the disease yourself, to help in this, and not to depress the body, as is often done.
В данный момент чувствую себя хорошо, настроение бодрое, надеюсь на выздоровление».
Это описание хорошо демонстрирует зависимость интерпретации ощущений от контекста, причем весьма трудно сказать, где конча ется миф и начинается реальность, когда ощущение «запускает» реальность, а когда под него подстраивается.
Хотя больная очень хорошо образованна, связь мифа и порож даемых им (или модифицируемых) ощущений мало отличается от случая «заболевания-змеи» в Корнуэлльсе, описанного Э.Б. Тайлором . Добавить к этому можно лишь то, что у больной все это время отмечалось прогрессирование заболевания.
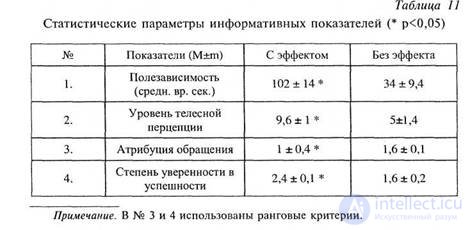
Наиболее информативными показателями, разделяющими больных с субъективным эффектом и его отсутствием при лече нии «катрексом», оказались следующее (по степени убывания информативности): степень полезависимости, уровень телесной перцепции, атрибуция обращения (сам больной добился включе ния его в группу для клинических испытаний или оно было ему предложено) и степень уверенности в эффекте лечения. В таблице 11 приведены статистические параметры этих показателей.
Рассмотрим последовательно каждый из информативных пока зателей. Для лучшей иллюстративности они будут представлены в графическом виде с использованием наиболее информативных гра даций разбиения распределений.
|
|
|
|
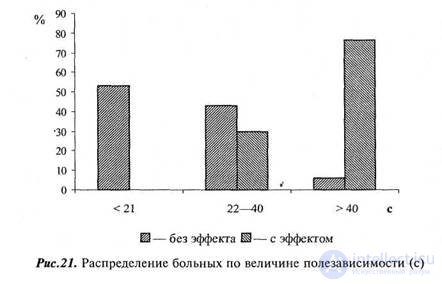
На рисунке 21 представлена диаграмма процентного распределения числа больных с субъективным эффектом и без эффекта лече ния по степени полезависимости. Связь этих параметров совершенно очевидна: высокополезависимые субъекты значимо чаще отмечают эффект лечения и уровень полезависимости является наиболее мощ ным фактором, определяющим эффект плацебо-лечения. Это впол не понятно, если учесть, что он характеризует фундаментальные принципы перцептивной стратегии: возможность вычленения сти мула из перцептивного поля, зависимость от условий предъявления
стимула и выбор системы координат — собственное тело или внеш нее окружение. Одна и та же концепция, даже если предположить одинаковую степень доверия к ней и равную степень усвоенности, будет обладать разными возможностями ее телесного подкрепления и проверки. Высокополезависимые лица легче игнорируют объек тивные характеристики стимула, демонстрируют большие пределы их искажения и, следовательно, лучшее подкрепление усвоенных мифологических конструкций и их меньшую верифицируемость.
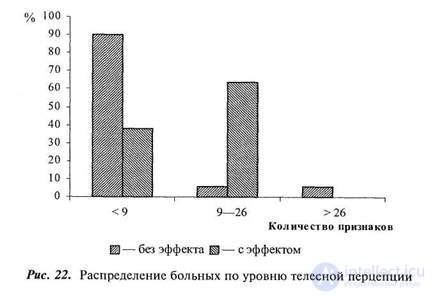
Однако сама возможность плацебо-лечения должна основы ваться на объективированных телесных ощущениях, на освоеннос ти языка тела. Очевидно, что чем этот язык богаче и сложнее и чем болезнь «артикулированнее», тем больше возможностей для оценки эффективности проводимой терапии. Как уже отмечалось, миф постоянно должен подпитываться реальностью, чтобы сохранять свое сходство с ней, и плацебо-лечение не меньше, чем истинное лече ние, должно подкрепляться телесным подтверждением. Поэтому не удивительно, что уровень вегетативной перцепции у больных с ус тойчивым субъективным эффектом значимо выше: они обладают исходно лучшими возможностями его оценить (рис. 22).
Уровень телесной перцепции отражает еще один интересный момент. В этот опросник включены, в основном, вегетативно регулируемые телесные функции и именно они, будучи телесно объективированными, преимущественно используются для оценки сома тического состояния. Поэтому снижение уровня тревожности и
|
|
улучшение психического состояния больных во время плацебо- лечения (если больной получает лечение, в которое он верит) при водит к нормализации вегетативных проявлений, рефлексирующихся лишь в их органной проекции, что расценивается больными как соматическое улучшение.
Полезависимость и уровень вегетативной перцепции отражают два автономных фактора субъективной эффективности лечения и практически не коррелируют друг с другом ( R = 0,133).
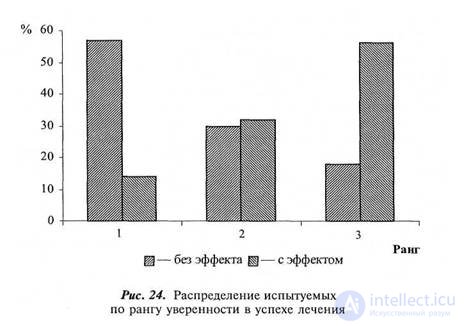
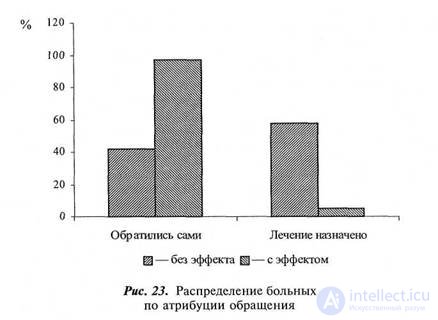
Более связаны между собой два следующих по степени инфор мативности показателя: атрибуция обращения и степень уверен ности в эффекте лечения ( R = 0,562; р < 0,05) (рис. 23, 24). Среди больных, обратившихся самостоятельно, эффект отмечается в 96 % случаев, а у тех, кому оно было рекомендовано, — лишь у 43 %. Точно так же, среди тех, кому лечение «катрексом», по их мне нию, помогло — 56 % высказывали до его начала полную уверенность в успехе, а среди тех, кому не помогло, — таких лишь 14%. В сущности, оба этих показателя отражают степень доверия к мифу на разных уровнях реализации: атрибуция обращения — на поведенческом, а степень уверенности — на вербальном. Поведен ческий уровень реализации более сложен, он включает в себя многие компоненты: стеничность, активность, объективные воз можности, но очень хорошо отражает истинную, а не деклариру емую уверенность в успехе (нужно очень верить в предполагав шийся успех, чтобы преодолеть все трудности, стоящие на пути его достижения). Менее показательны в этом отношении больные, которым лечение рекомендовалось врачом: в этом случае степень уверенности самого пациента в успехе лечения не имела принци пиального значения.
Итак, полученные результаты доказывают, что эффект мифо логизированной процедуры лечения в значительной степени опре деляется такими индивидуально-психологическими характеристика ми как полезависимость / поленезависимость, уровень вегетативной (или, более точно, телесной) перцепции и степень доверия к ми фологическому концепту. Это еще одно доказательство того, что величина плацебо-эффекта не является неким стабильным парамет ром и не может применяться в качестве универсального показателя без учета формирующих его факторов.
Можно с большой степенью уверенности сказать, что высоко полезависимый субъект получит ощущение улучшения от любого вида лечения, если будет в него верить и выберет его сам. Само же содержание лечения и его обоснованность не имеют для достиже ния субъективного эффекта практически никакого значения. it
|
|
простое правило было бы полезно конкретизировать, установив формализованные граничные критерии.
Таким практическим следствием стала разработка с помощью экспертной системы решающего правила, которое на основании небольшого количества показателей позволяет предсказать результат плацебо-лечения. При выборе показателей мы старались максимально упростить необходимое для этого психологическое обследование, сделав
|
|
его доступным для любого пользователя. В результате мини мизации измерений было построено два таких решающих правила.
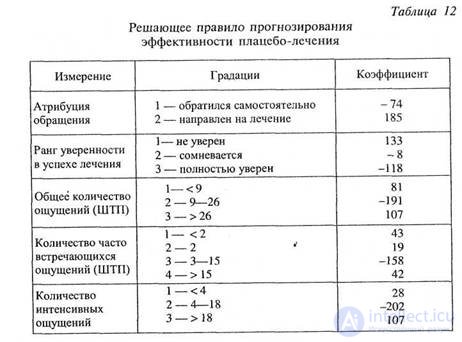
В первое, прогнозирующее отрицательный результат с вероятностью 90,5 %, а положительный с вероятностью 84,4 %, вошло 5 показателей: атрибуция обращения, степень уверенности в эффекте, уровень вегетативной перцепции (а — общий объем испытываемых ощущений, б — количество часто испытываемых ощущений, в — количество интенсивных ощущений). Пользоваться решающим правилом необходимо следующим образом. Все измере ния разбиты на информативные градации, каждой из которых присвоен определенный коэффициент (табл. 12). Определив, в какие градации попадают измерения, необходимо суммировать коэффициенты. Если их сумма S > 0, то с вероятностью 90,5 % у
данного субъекта плацебо-лечение не будет эффективным, а если S < 0, то с 84,4 % вероятностью субъективный эффект будет.
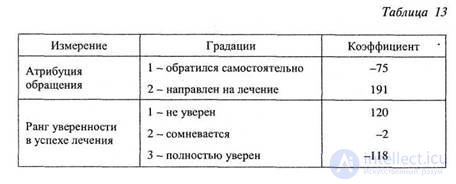
С некоторыми потерями в точности решающее правило можно еще упростить, оставив лишь два признака: атрибуцию обращения и степень уверенности (табл. 13). Правило пользования остается тем же, но в этом случае эффективность можно будет предсказать с ве роятностью 85,3 %, а ее отсутствие, — с вероятностью 71,4%.
Разработанное решающее правило может найти широкое применение в клинической практике, отборе больных для психотерапии, клинических испытаниях новых препаратов и методов лечения, а также при рандомизации исследований.
Итак, полученные результаты доказывают, что эффект мифологизированной процедуры лечения в значительной степени опре деляется такими индивидуально-психологическими характеристи ками, как полезависимость / поленезависимостъ, уровень телесной перцепции и степень доверия к мифологическому концепту. Величина плацебо-эффекта не является неким стабильным параметром и не может применяться в качестве универсального показателя без учета формирующих его факторов.
Этот тезис имеет вполне конкретные практические следствия, так как существует очевидная возможность улучшить показатели любой терапевтической процедуры, повысив ее эффективность за счет семиотических компонентов.
As we have seen in the study, the most important is the degree to which the client believes the proposed concept-myth. This opens up ample opportunities for manipulating trusting clients and creating a convincing image of a qualified healer. Detailed instruction of the patient is very effective, giving him the language necessary for fixing and realizing the possible effect, and the introduction of a system for mediating his bodily functions. Thus, the task of false biofeedback increases the number of placebo-phenomena by 2-3 times (Tkhostov, 1991).
A special way of ensuring customer confidence is the introduction of treatment fees. This at the same time achieves the solution of two tasks: increasing the prestige of treatment (the high price seems to guarantee the quality of services) and, more importantly, instantly eliminating unmotivated and insufficiently trusting clients. Paid treatment is a hidden and very accurate implementation of the attribute treatment. The amount of payment that the client is ready to make can be considered as a measure of his motivation. With known reservations, this is very similar to the method of measuring the severity of a rat’s needs by the magnitude of an electric current that it was able to undergo to achieve a stimulus, as practiced in experimental psychology. From a semiotic point of view, paid treatment always has advantages over free treatment. Equally obvious is the role of selecting motivated and trusting patients by the need for a long wait, pre-recording. The queue clarifies the attribution of the appeal and, like high fees, increases the authority of the doctor. In the apocryphal stories about the work of V.M. Bekhtereva has a very interesting description of what he took for treatment for alcoholism only those who begged him to do so on his knees. Even if this is not true, by itself the principle of such a selection would certainly be more than effective.
Focusing on motivated and trusting patients can also explain the sectarian hue of the activities of every popular psychotherapist: the requirement of complete submission, the position of the guru-teacher, who owns the most intimate knowledge, hard screening of doubters and dissidents. If, for example, we turn to the history of psychoanalysis, not to mention the less reflective psychotherapeutic techniques, then one cannot fail to notice that its development was usually accompanied by constant schisms and scandals: the trial between 3. Freud and C. Jung, exile of J. Lacan from the International Psychoanalytic Association, etc.
The semiotic efficacy of the treatment process can also be significantly improved if selected for the treatment of individuals with a high degree of field dependence and a well-developed ability to distinguish and reflex subjective sensations (or create conditions for their generation in one way or another). The degree of field dependence increases when taking drugs, alcohol, psychotropic drugs, prolonged hyperventilation, which is widely used in shamanic practice and traditional medicine.
Very interesting are the yoga techniques associated with fixing attention on your body, original methods of its objectification, controlled breathing, and mastering body language. Modern methods of body-oriented psychotherapy using similar mechanisms are quite close to them. In my opinion, the most popular method of holotropic breathing according to Stanislav Grof is especially destructive. The old hyperventilation technique underlying it, generating hypocapnic phenomena and dysfunction of vegetative regulation, accompanied by abundant bodily sensations and changes in the state of consciousness (Moldovan , 1991), at the same time leads to a sharp increase in field dependence. Methods of this kind themselves simultaneously create phenomena that reinforce the mythological constructions built over them and conditions that complicate their testing. The effectiveness of techniques of this kind is rather difficult to question, since they are based on closed structures, the mythological nature of which is imperceptible but very firmly rooted in a phenomenologically obvious reality.
The strength of the mythological constructions of psychotherapeutic practice, ensuring the success of their application, leads to significant difficulties in its scientific understanding. A variety of treatment philosophies, almost equal to the effectiveness of different psychotherapeutic processes, obscure the underlying structural unity. It is very difficult for a psychotherapist to understand and even less to recognize that the originality of the method he has suffered from a scientific point of view has nothing more than an ethnographic value and its advantages over a shaman are very relative. Receiving constant confirmation of the effectiveness of his method (no matter how absurd it may be - every psychotherapist will find his client), he is inclined to fall into “Quevalidism” - faith in his own exclusiveness, the reality of the “original” theoretical constructs.
Combined with the obvious anti-scientist and pragmatic attitudes of modern society and some scientists, this trend becomes extremely dangerous. “If we take the practice directly (pre-theoretically), then successful practice confirms the existence of such objects and their special chronotopes as“ evil spirits ”” (Tishchenko, 19916, pp. 21-22). A psychotherapist or psychologist, who follows his practice and does not want to notice that this practice can generate semiotic fan toms with all the signs of reality, is doomed to live in this phantom world. He, of course, has this right, but it must be borne in mind that the psychotherapist's personal conviction of the truth of his theory and the commercial success of his work are insufficient arguments for science.

Comments
To leave a comment
The psychology of corporeality
Terms: The psychology of corporeality